
Are Younger Generations Really Aging Faster Or Are We Watching Something Else Entirely?
We maybe watching metabolic disease consume the body’s repair capacity at a rate the previous generation never faced.

OPINION PIECE
On June 22, 2026, Nature Medicine published a study from a team at Washington University School of Medicine in St. Louis reporting that younger adults are aging biologically faster than older adults born decades earlier, and this accelerated aging is linked to the rising incidence of early-onset solid cancers (Tian et al., 2026). The WashU press release described the finding as a possible biological explanation for why cancer is increasingly striking people under 50, treating “accelerated aging” as the new headline phenomenon.
When I read the paper carefully and against the broader literature on metabolic disease, inflammation, and aging biology, I came away with a very different impression of what is actually being measured. What follows is my interpretation of the evidence, not the conclusions the authors expressed on the original paper. I think the standard framing misses what may be the most important thing about this finding.

What the Paper Actually Shows
The Tian study analyzed 154,169 participants in the United Kingdom (UK) Biobank and 10,262 participants in the United States National Institutes of Health (NIH) All of Us Research Program. The team used three biological aging metrics: PhenoAge, the Klemera-Doubal Method (KDM), and a metabolomic age score. They calculated each participant’s “age gap,” the difference between biological and chronological age, and then prospectively linked the age gap to incident early-onset solid cancers in people under 55.
Each one standard deviation increase in PhenoAge gap was associated with an 8% increase in early-onset cancer risk (hazard ratio 1.08), and people in the highest tertile of biological aging had a 15% higher risk than those in the lowest tertile. The three aging metrics produced directionally consistent but variable results. Organ-specific analyses linked immune-system aging to lung cancer risk and adipose-tissue aging to colorectal cancer risk. The All of Us cohort produced partial replication based on only 104 incident cases over an average follow-up of 2.4 years. The authors appropriately acknowledged that an observational design cannot establish causation.
Two independent senior investigators commented on the paper through the United Kingdom (UK) Science Media Centre on the day of publication. Dr. Jyoti Nangalia of the Wellcome Sanger Institute raised the central methodological question directly: are these biological age measurements capturing processes that drive cancer, or are both the aging changes and the cancer being driven by other shared upstream factors (Science Media Centre, 2026)? That question, posed at the moment of publication by a senior cancer geneticist, is the question this article addresses.
What PhenoAge Is Built From
PhenoAge, the aging clock most central to the Tian analysis, is built from nine blood biomarkers: albumin, alkaline phosphatase, creatinine, C-reactive protein (CRP), glucose, mean cell volume (MCV), red cell distribution width (RDW), white blood cell count (WBC), and lymphocyte percentage (Levine et al., 2018). Look at that list and ask the diagnostic question a clinician asks every day: what conditions move these numbers?
CRP is the prototypical marker of chronic low-grade inflammation, and it is elevated in obesity, metabolic syndrome, and type 2 diabetes. Fasting glucose is, by definition, the variable that defines dysglycemia. Albumin falls in chronic inflammatory states and in hepatic dysfunction associated with metabolic-associated steatotic liver disease. Alkaline phosphatase is elevated in fatty liver disease. WBC count rises with chronic inflammation. RDW rises with metabolic and cardiovascular dysfunction. Lymphocyte percentage shifts with chronic immune activation. MCV moves with nutritional status and chronic disease.
Every single one of these nine biomarkers is directly moved by metabolic disease and its inflammatory consequences. PhenoAge is not measuring some abstract aging biology, is measuring a composite of inflammation, glycemic dysregulation, and the visceral footprint of metabolic dysfunction, packaged as a single number and labeled “biological age”.
If you accept that framing, the question is no longer if younger generations are aging faster? The question becomes; are younger generations carrying a higher metabolic-inflammatory burden than their parents and grandparents did at the same age, and is that burden showing up in the biomarkers we use to estimate aging? The literature answers that question with a clear yes.
Metabolic Disease Moves the Aging Clock
The published literature on metabolic syndrome and biological aging is large and remarkably consistent across cohorts, aging clocks, and age ranges.
McCarthy and colleagues, working in the Irish Longitudinal Study on Ageing (TILDA), examined 469 participants and found that metabolic syndrome was associated with accelerated epigenetic aging as measured by the GrimAge clock. Critically, the team performed a mediation analysis and found that CRP, the inflammatory marker, mediated approximately one-third of the metabolic-syndrome-to-aging association (McCarthy et al., 2024).
Föhr and colleagues conducted a twin study published in the International Journal of Obesity, examining 268 participants in the discovery cohort with replication in 1,857 additional participants across ages 23 to 69. Metabolic syndrome was associated with acceleration on both the GrimAge clock and the DunedinPACE clock. The twin design is what makes this study particularly informative. By comparing twins discordant for metabolic syndrome, the investigators could partially separate genetic susceptibility from the metabolic exposure itself. Shared genetic factors explained much of the GrimAge association, but the DunedinPACE association persisted within twin pairs (Föhr et al., 2024). Some of what aging clocks detect is genetic susceptibility shared with metabolic disease, the rest is the metabolic process itself.
Lemke and colleagues, working in the Coronary Artery Risk Development in Young Adults (CARDIA) cohort, conducted a longitudinal analysis directly relevant to the age range of the Tian paper. Metabolic syndrome severity prospectively predicted epigenetic age acceleration in young adults. The authors framed accelerated epigenetic aging as a potential early-detection tool for emerging metabolic syndrome (Lemke et al., 2019). In other words, the people studying aging clocks in young adults already proposed, in 2019, that what the clocks are reading is essentially the metabolic process.
Davis and colleagues examined 273 children aged 8 to 14 and found that higher body mass index (BMI) was associated with accelerated epigenetic aging (Davis et al., 2022). Salech and colleagues, working in a Chilean cohort, reported that persistent obesity since childhood and adolescence was associated with accelerated biological aging in young adults (Salech et al., 2024). The metabolic-to-aging association is detectable before adolescence and tracks forward through the young adult years where the Tian paper finds its strongest evidence.
If you enjoy evidence-based medical information, subscribe to receive these articles delivered to your mailbox every week.
Chronic Inflammation as the Connector
The biological link between metabolic dysfunction and accelerated aging is chronic low-grade inflammation. This pathway is well documented. Tam and colleagues, in a 2024 review in Immunity & Ageing, traced the chain: obesity drives adipocyte senescence; senescent adipocytes propagate the senescence-associated secretory phenotype (SASP) to immune cells; chronic low-grade inflammation results; this inflammation feeds back to worsen metabolic dysfunction and accelerates the cellular processes that aging clocks detect (Tam et al., 2024).
Liu and colleagues, in a 2025 review in Cell Death Discovery, catalogued ten overlapping mechanisms between obesity and aging: systemic inflammation, telomere depletion, epigenetic alterations, mitochondrial dysfunction, stem cell exhaustion, deregulated nutrient sensing, genomic instability, loss of cellular homeostasis, accumulation of senescent cells, and gut dysbiosis (Liu et al., 2025). Obesity essentially recapitulates the hallmarks of aging at the molecular level. The 2014 foundational review by Park and colleagues in Inflammation Research had already established the reciprocally reinforcing relationship between age-related inflammation and insulin resistance (Park et al., 2014).
The inflammaging literature, beginning with Franceschi’s foundational 2000 paper in the Annals of the New York Academy of Sciences and extending forward for two decades, has established that chronic low-grade inflammation is itself a fundamental driver of aging biology (Franceschi et al., 2000). What is new is the recognition that the generational rise in metabolic disease has loaded younger cohorts with this inflammatory burden earlier in life than their parents carried it.
The Same Mechanism Drives Early-Onset Cancer
The metabolic-inflammatory axis is independently established as a driver of early-onset cancer, particularly early-onset colorectal cancer.
Liu and colleagues, in a 2024 review in Frontiers in Oncology, argued explicitly that obesity-induced low-grade inflammation may play a more important role in early-onset colorectal cancer than in late-onset disease (Liu et al., 2024). Schumacher and colleagues, in a 2024 paper in Cancers, identified tumor-associated macrophage metabolism, leptin and adiponectin signaling, and the PI3K/AKT pathway as the specific biology linking obesity to early-onset colorectal cancer (Schumacher et al., 2024). Kühn and colleagues, in a 2017 nested case-control analysis using prediagnostic samples from the Västerbotten Intervention Programme, showed that the association between metabolic syndrome and colorectal cancer is substantially mediated by inflammatory proteins, with visceral adiposity as the driving exposure (Kühn et al., 2017).
The clearest statement comes from a paper the Tian team cites in their own reference list. Du and colleagues, in a 2025 review in Nature Reviews Endocrinology, reframe early-onset colorectal cancer explicitly as a disease of metabolic dysregulation (Du et al., 2025). The Tian authors cite this paper to explain why their adipose-aging-to-colorectal-cancer finding is biologically plausible.
Younger birth cohorts carry higher rates of obesity, metabolic dysfunction, and chronic inflammation than their parents and grandparents did at the same age. These conditions move the biomarkers that aging clocks are built from. These same conditions independently drive early-onset cancer through documented mechanisms. The accelerated aging finding and the early-onset cancer finding are not two separate phenomena requiring two separate explanations. They are the same epidemiologic phenomenon observed through two different windows.
The Osteoarthritis Parallel
I find it useful to think about this through a parallel to a disease most readers know. Osteoarthritis (OA) of the elderly is conventionally understood as a wear-and-tear phenomenon. The articular cartilage that lines joint surfaces has bounded capacity to repair the microscopic damage that ordinary mechanical loading produces over a lifetime. Repair keeps pace with damage for decades, until late in life, when accumulated microscopic damage finally exceeds repair capacity and the clinical picture of OA emerges.
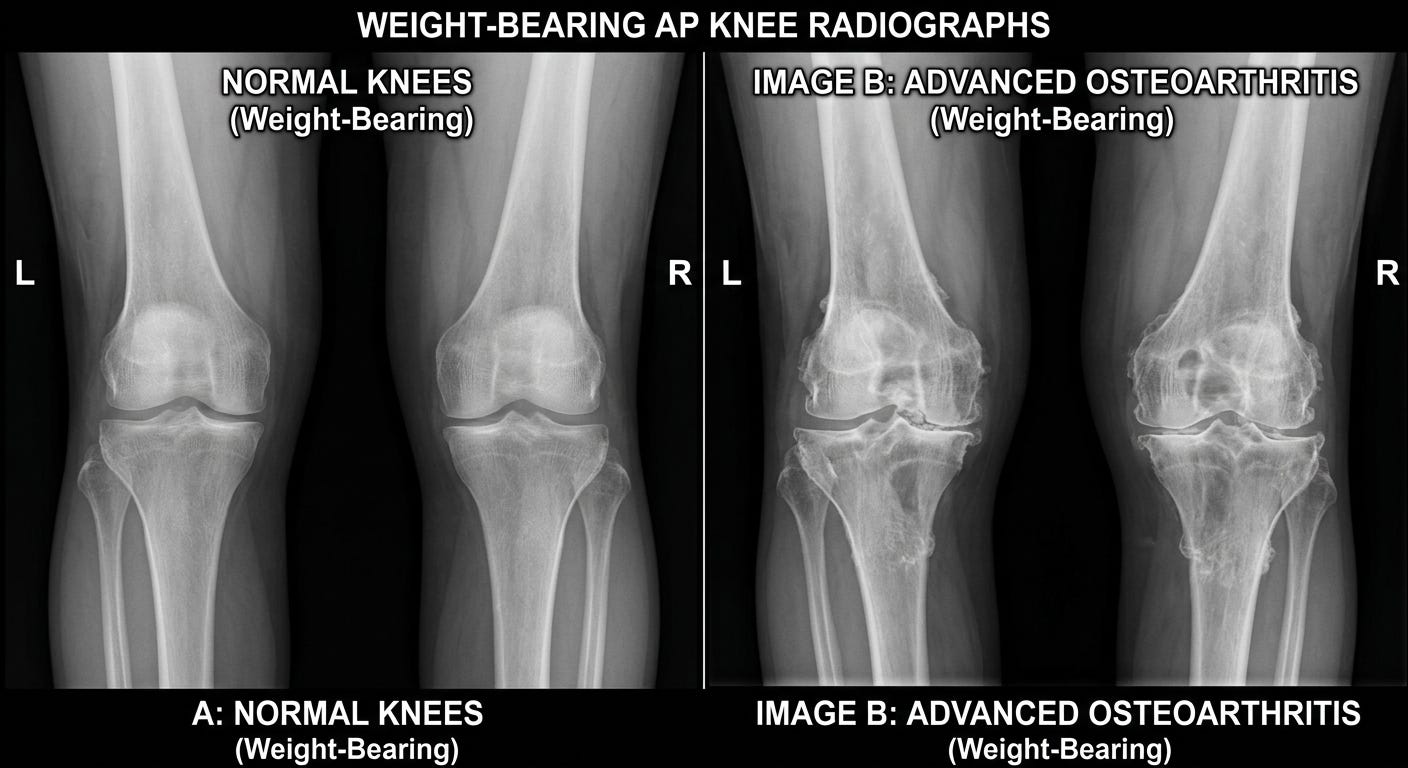
In some populations, the timeline collapses. The competitive runner with thirty years of high-mileage training presents with OA in their forties, not their seventies. The patient who has carried 100 extra pounds for two decades presents with knee OA in their fifties. Same disease, same mechanism, different timeline, driven entirely by the rate of damage accumulation relative to the bounded rate of repair.
The same logic applies to systemic biology. The body’s cellular repair systems operate at roughly bounded rates. Chronic metabolic-driven inflammation produces continuous low-grade damage across multiple systems simultaneously. When the rate of accumulation chronically exceeds what ongoing repair can keep up with, the failure modes ordinarily associated with old age, including cancer, appear earlier.
This is a conceptual frame, not a documented pathway. It aligns with established theoretical work: the disposable soma theory of aging, the inflammaging framework, the cumulative damage model. I offer it as a useful lens for thinking about what is happening, not as a finding.
The Integrative Principle
Modern biomedical science studies aging in one discipline, metabolic disease in another, oncology in a third, and inflammation in a fourth. Press coverage and clinical practice tend to inherit this fragmentation; the Tian paper is a case in point. It is excellent aging-epidemiology work that, viewed through the wider lens of metabolic medicine and inflammation biology, reveals something other than what its framing suggests.
Aging is not an independent, autonomous process happening on its own clock. It is the integrated consequence of how every other system in the body is functioning over time. The aging researchers are not wrong to study aging as an independent phenomenon, this is useful for the organization of research itself. They become misleading when imported into public understanding of how the body actually works. A finding that the same nine inflammatory and metabolic biomarkers move with both “accelerated aging” and early-onset cancer should not surprise anyone. It is the same biology, named differently in different disciplines.
This recognition transforms the conversation about metabolic health. Improving metabolic health is not merely about getting the glucose, blood pressure, and weight on the scale into normal range, important as those targets are. It is about reducing the cumulative inflammatory burden that is reshaping the trajectory of biological aging itself and increasing susceptibility to the diseases conventionally associated with old age.
The Impact in Real Numbers
The numbers that frame this for the United States are clinically sobering. According to the Centers for Disease Control and Prevention (CDC), approximately 38% of American adults have prediabetes and another 11% have diagnosed or undiagnosed diabetes, meaning roughly half the adult population is somewhere on the dysglycemia spectrum (CDC, 2024). The American Heart Association reports that more than one in three American adults meet the criteria for metabolic syndrome (American Heart Association, 2024). The economic burden is comparably large. The American Diabetes Association estimates the total annual cost of diabetes in the United States at $413 billion as of the most recent national accounting (American Diabetes Association, 2024).
The early-onset cancer trend that the Tian paper attempts to explain is real and accelerating. Early-onset colorectal cancer incidence in particular has been rising for three decades, and Berrington de Gonzalez and colleagues, in a 2025 international comparative analysis published in the Annals of Internal Medicine, documented similar trends across multiple high-income countries (Berrington de Gonzalez et al., 2025). These are the same countries in which the metabolic-disease curve has been climbing for the same period. The temporal correlation does not prove causation, but it is the kind of correlation a metabolic-inflammatory explanation predicts and the kind a sealed-off “accelerated aging” explanation does not.
What This Means For You
The same lifestyle modifications this publication has covered repeatedly, and will continue to cover, are not just about preventing the diseases of metabolic dysfunction. They are about reducing the rate at which the cumulative damage that accelerates biological aging accumulates. The action steps are familiar, and they are the right ones:
Reduce ultraprocessed food consumption, which independently drives inflammation, dysglycemia, and weight gain. The single highest-yield change in the contemporary American food environment is reducing the share of calories coming from industrially formulated foods.
Eat a dietary pattern centered on whole foods, with abundant vegetables, legumes, intact whole grains, nuts, fish, and olive oil, in the Mediterranean tradition. This pattern has the strongest evidence base for reducing inflammatory and metabolic markers.
Move daily: both aerobic activity and resistance training independently improve insulin sensitivity, reduce inflammatory markers, and preserve the metabolic flexibility that decays with age and metabolic disease.
Sleep seven to nine hours per night on a regular schedule. Sleep restriction directly impairs glucose tolerance and raises inflammatory markers within days.
Address chronic psychological stress, which directly elevates cortisol and inflammatory cytokines and indirectly drives the behaviors that worsen metabolic health.
Eliminate tobacco and treat alcohol intake as a metabolic exposure to be minimized, not a neutral social variable.
None of this is new information, what may be new is the reason to take it seriously.
Aging is not something that simply happens to us on a clock we do not control. It is in substantial part something we accelerate or decelerate through how we live, beginning earlier than most of us realize and continuing through every decade that follows.
Found this article useful? Share your thoughts. Join the conversation below.
Educational content on The Metabolic Archives is free, because medical information should be accessible to everyone. If you find value and want to support the work, a paid subscription is available and genuinely appreciated. Visit the About Page for additional information.
The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.