
Berberine, Nature’s Ozempic?
What the science actually shows and what the wellness industry is not telling you about the risks

What Berberine Is
Berberine is a plant alkaloid, a class of nitrogen-containing compounds that plants produce not for human benefit but as chemical defense mechanisms against insects, herbivores, and microbial pathogens. It is found in the roots, bark, and stems of several plant species, including Berberis vulgaris (barberry), Coptis chinensis (goldenseal’s Asian relative), and Hydrastis canadensis (goldenseal itself).
Its history of human use spans approximately 3,000 years in traditional Chinese medicine and Ayurvedic practice, almost entirely as an antimicrobial. It was used for gastrointestinal infections, wound treatment, and diarrheal illness. The metabolic applications are entirely modern, and they were discovered accidentally: Chinese physicians treating diabetic patients with berberine-containing herbal preparations in the 1980s noticed unexpected improvements in fasting glucose. That observation eventually prompted systematic investigation.
The Bioavailability Problem
Oral bioavailability is under 1% in humans (Expert Opinion on Drug Metabolism and Toxicology, 2023). Following a standard 300mg dose, peak plasma concentration reaches approximately 0.33 micrograms per liter. Approximately 99.5% of an oral berberine dose is eliminated during gastrointestinal first-pass processing, through a combination of P-glycoprotein-mediated efflux, extensive intestinal and hepatic first-pass metabolism by cytochrome P450 (CYP) enzymes, and low membrane permeability.
Because berberine is poorly absorbed, it accumulates at very high concentrations in the gastrointestinal (GI) tract before the small fraction that survives first-pass metabolism enters systemic circulation. High local concentrations act directly on intestinal enzymes involved in carbohydrate digestion, on enteroendocrine cells that secrete gut hormones, and on the gut microbiome.
Metformin, the best-characterized oral diabetes medication available, works through a strikingly similar model. Metformin accumulates in intestinal epithelial cells at concentrations far exceeding plasma levels, stimulates GLP-1 secretion from enteroendocrine L-cells in the distal gut, alters bile acid metabolism, and remodels the gut microbiome, particularly increasing Akkermansia muciniphila (McCreight et al., Diabetologia, 2016). A delayed-release metformin formulation achieves comparable glycemic control to immediate-release with significantly less systemic exposure, a finding that supports the gut as a primary site of action rather than systemic circulation. Berberine and metformin share this gut-predominant profile and produce overlapping microbiome changes.
Dihydroberberine and phytosome-complexed berberine products claim improved bioavailability. The problem is that improved systemic absorption does not come with clinical outcome evidence demonstrating better results. The formulation claims are ahead of the evidence and the safety implications of enhanced bioavailability are genuinely unknown.
What the Science Actually Shows
Glucose Lowering
Multiple meta-analyses demonstrate significant reductions in fasting plasma glucose (weighted mean difference of approximately -0.515 mmol/L) and two-hour oral glucose tolerance test (OGTT) glucose (weighted mean difference of approximately -1.606 mmol/L) compared to placebo in metabolic syndrome and type 2 diabetes mellitus (T2DM) populations.
The most frequently cited head-to-head trial compared berberine directly to metformin in 116 patients with T2DM over 13 weeks (Yin et al., Metabolism, 2008). Both produced approximately 2 percentage point reductions in glycated hemoglobin (HbA1c). A 2023 meta-analysis in JAMA Network Open confirmed comparable glucose lowering across multiple trials.
The evidence comes overwhelmingly from Chinese populations with established T2DM who were simultaneously implementing lifestyle modification. The contribution of concurrent lifestyle change to the observed outcomes cannot be cleanly separated from berberine’s pharmacological effect. Western, non-diabetic populations are not adequately represented in the evidence base.
The head-to-head trials are open-label, small-sample, and short-duration. The glucose-lowering effect is a real finding in a specific population under specific conditions.
Lipid Modulation
Berberine produces consistent reductions in low-density lipoprotein cholesterol (LDL-C) (weighted mean difference approximately -0.495 mmol/L), total cholesterol (approximately -0.451 mmol/L), and triglycerides (approximately -0.367 mmol/L) compared to placebo. High-density lipoprotein cholesterol (HDL-C) is not significantly affected.
The mechanism responsible for LDL-C reduction includes upregulation of LDL receptor expression through inhibition of proprotein convertase subtilisin/kexin type 9 (PCSK9). PCSK9 is the same target as evolocumab and alirocumab, two injectable monoclonal antibodies that represent some of the most expensive cholesterol medications available (Kong et al., Nature Medicine, 2004). Berberine achieves PCSK9 inhibition through a different mechanism than these biologics.
A 2023 meta-analysis of 44 randomized controlled trials (RCTs) found that berberine alone showed no significant lipid benefit compared to statins or standard care, with very high heterogeneity across trials (I-squared of 76-96%) (Yang et al., Phytomedicine, 2023). Berberine reduces lipids compared to placebo.
Weight and Body Composition
A 2025 meta-analysis of 23 RCTs found statistically significant reductions in body weight (mean difference -0.88 kg), body mass index (BMI) (mean difference -0.48 kg per square meter), and waist circumference (mean difference -1.32 cm), but no significant reduction in waist-to-hip ratio, suggesting minimal specific effect on visceral fat (International Journal of Obesity, 2026).
The most plausible interpretation is that the modest weight effect is secondary to metabolic improvement rather than a primary fat-loss mechanism. Berberine is not acting on appetite regulation, energy expenditure, or adipose tissue biology in any way that resembles GLP-1 receptor agonism.
Gut Microbiome
Berberine increases certain bacterial species in the gut, particularly Akkermansia muciniphila, through an indirect mechanism involving gut mucin secretion and alterations in the intestinal environment produced by its antimicrobial activity and metabolic effects (Xie et al., Microbiology Spectrum, 2025). Akkermansia muciniphila is associated with metabolic health in observational data. The human evidence for clinically meaningful microbiome benefit from berberine supplementation remains limited. The marketing extrapolation from a specific mechanistic finding to a general wellness claim is not supported.
If you enjoy evidence-based medical information, subscribe to receive these articles delivered to your mailbox every week.
Cancer Claims
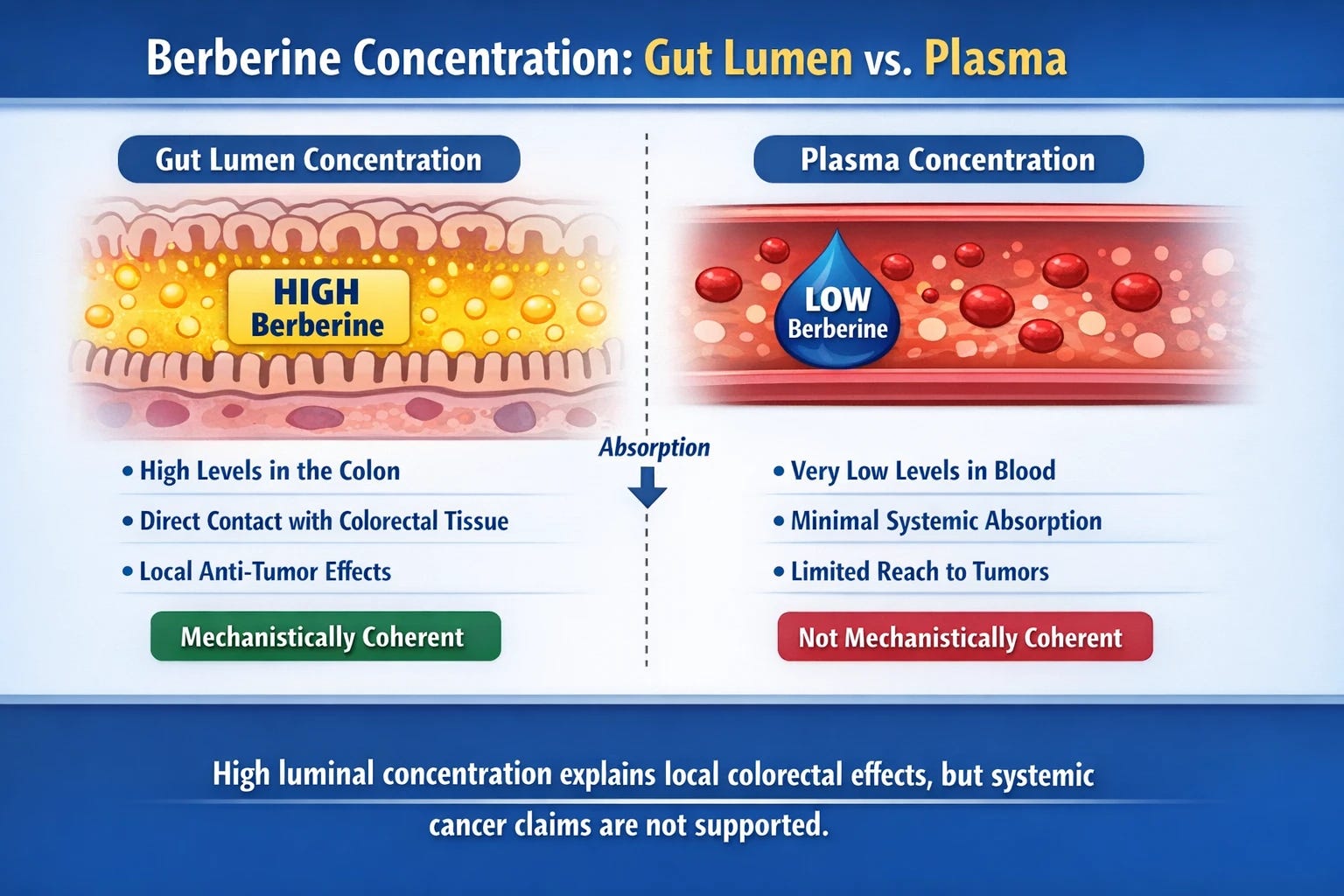
Almost all of berberine’s marketed cancer claims are based on cell culture experiments using concentrations that cannot be achieved in human tissue at standard oral doses. Given that less than 1% of berberine reaches the bloodstream, the plasma concentrations that might be relevant to systemic tumor biology simply do not materialize.
Colorectal adenoma chemoprevention is the strongest evidence berberine has in any clinical application, and the mechanism is coherent. A multicenter, double-blind RCT enrolled 1,100 Chinese post-polypectomy patients and found that berberine 0.3g twice daily reduced adenoma recurrence by 23% relative risk reduction at two years compared to placebo (Chen et al., Lancet Gastroenterology and Hepatology, 2020). A 2025 six-year follow-up study of the same cohort found durable protection persisting after treatment cessation: adenoma recurrence occurred in 34.7% of the berberine group versus 52.1% in the placebo group, with neoplasm occurrence also lower in the berberine arm (Tan et al., Lancet Regional Health, Western Pacific, 2025).
The compound does not need systemic absorption to act on colonic mucosa. The bioavailability problem that undermines systemic cancer claims is the same pharmacokinetic feature that makes colorectal adenoma chemoprevention biologically plausible.
The Honest Comparison: Metformin
Berberine and metformin share mitochondrial respiratory complex I inhibition in intestinal epithelium as a core mechanism for glucose lowering. Berberine’s glucose-lowering effect includes both AMP-activated protein kinase (AMPK)-dependent and AMPK-independent pathways: complex I inhibition drives glycolysis stimulation directly, with AMPK activation as a consequence rather than the primary mechanism (Liu et al., Journal of Cellular and Molecular Medicine, 2018). Both compounds work predominantly in the gut. Both increase Akkermansia muciniphila. Both reduce fasting glucose and HbA1c in T2DM populations. Short-duration head-to-head trials show comparable surrogate endpoint effects.
Metformin has decades of cardiovascular outcome data, including the United Kingdom Prospective Diabetes Study (UKPDS), which demonstrated reduction in macrovascular endpoints in overweight T2DM patients. No equivalent hard outcome data exists for berberine. No myocardial infarction, stroke, or mortality endpoint trial has been completed. A Mendelian randomization study using UK Biobank data found that a berberine biological response was associated with reduced risk of ischemic heart disease (odds ratio 0.85, 95% CI 0.79-0.91) and diabetes (odds ratio 0.88, 95% CI 0.80-0.96) (Zhao et al., npj Cardiovascular Health, 2026). Mendelian randomization provides stronger causal inference than standard observational data, but it does not substitute for a randomized outcome trial.
Metformin is manufactured under Food and Drug Administration (FDA) regulatory oversight to standardized pharmaceutical specifications, berberine supplements are not. Metformin is frequently covered by insurance when prescribed, berberine supplements are not. Metformin is available as a generic for under $10 per month.
For every metabolic indication where berberine is being marketed, metformin is a thoroughly characterized, FDA-regulated, generically available alternative that any physician will readily prescribe if clinically indicated. The comparison between them is not close.
Adverse Effects and Drug Interactions
Gastrointestinal Effects
GI side effects are the most common adverse effects of berberine: nausea, constipation, diarrhea, abdominal cramping, and flatulence. They are usually dose-dependent and self-limiting, and they parallel the GI side effect profile of metformin. For most people, they are manageable.
A Theoretical Concern Grounded in Mechanism
Berberine, metformin, and phenformin, a biguanide withdrawn from clinical use in the 1970s, all inhibit mitochondrial complex I as a shared mechanism. Phenformin was withdrawn because it produced unacceptable rates of lactic acidosis, a life-threatening complication of impaired lactate clearance when mitochondrial function is suppressed. Metformin produces lactic acidosis at a far lower rate, which is why it remains in use, but the FDA mandates contraindication in patients with renal impairment, hepatic insufficiency, or conditions associated with tissue hypoperfusion, precisely because these states reduce the safety margin around complex I inhibition.
Berberine produces dose-dependent lactate elevation consistent with complex I inhibition (Oncotarget, 2018). No documented human case of berberine-associated lactic acidosis exists in the literature. This is a theoretical concern grounded in mechanism but it is a concern that demands specific attention for patients with renal impairment, hepatic insufficiency, or tissue hypoperfusion, and for anyone considering high-bioavailability formulations whose systemic exposure profile has not been safety-characterized. These patients are not candidates for self-directed berberine supplementation.
The Real Health Concern
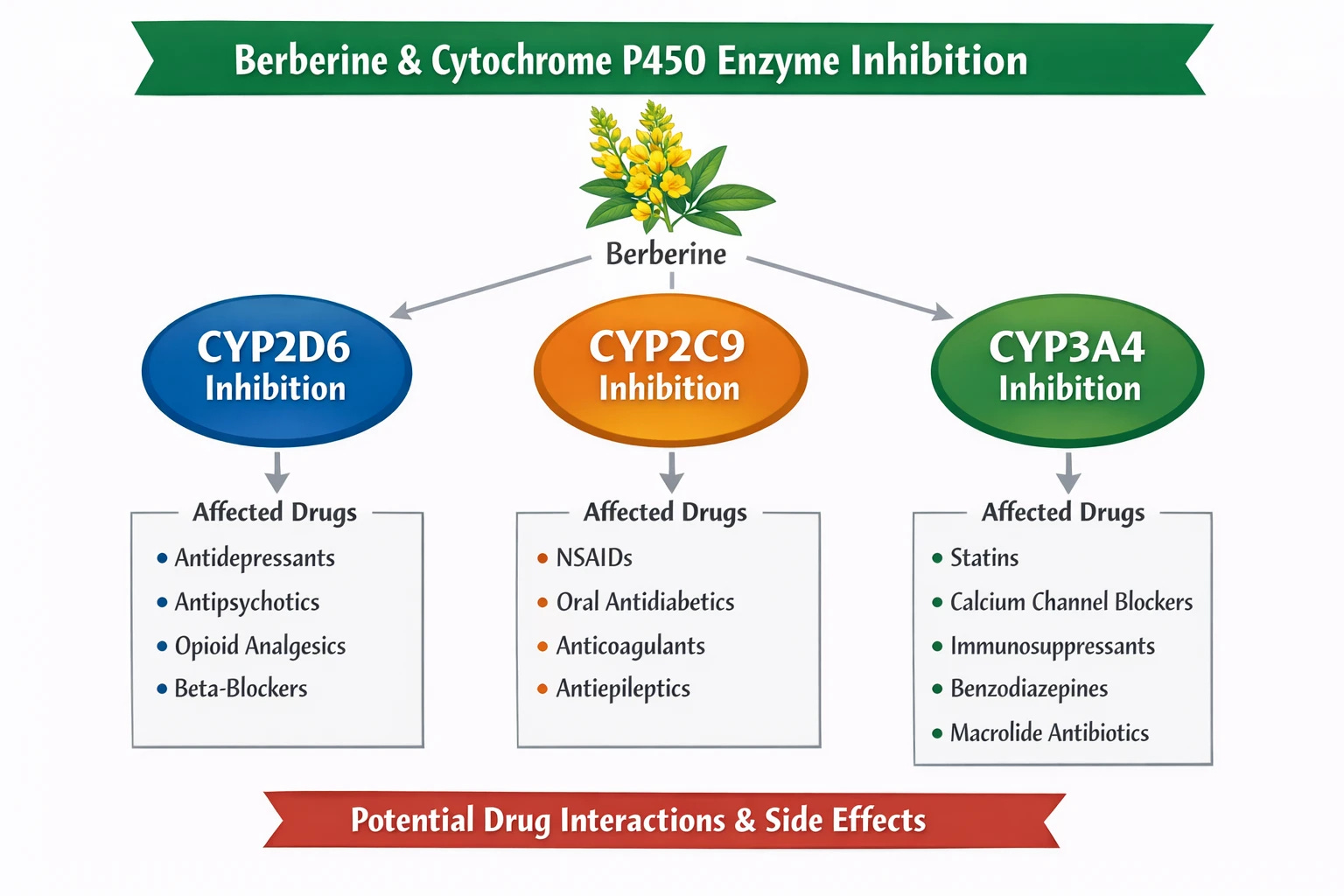
Berberine is a potent inhibitor of several cytochrome P450 (CYP) liver enzymes, the enzyme family responsible for metabolizing the majority of pharmaceutical drugs in common use. When these enzymes are inhibited, medications that depend on them for clearance accumulate to higher plasma concentrations than intended. Depending on the drug involved, that accumulation can range from clinically inconsequential to life-threatening.
A randomized crossover study in healthy volunteers receiving berberine 300mg three times daily for two weeks demonstrated a ninefold increase in the urinary dextromethorphan/dextrorphan ratio, a validated measure of CYP2D6 inhibition, and a twofold increase in the losartan/E-3174 ratio, a validated measure of CYP2C9 inhibition (Guo et al., European Journal of Clinical Pharmacology, 2012). P-glycoprotein inhibition and CYP3A4 inhibition have been demonstrated at doses as low as 300mg per day in cyclosporine interaction studies (Xin et al., 2006).
The clinical implications depend on which medications are involved:
Warfarin and anticoagulants. Berberine inhibits the CYP2C9-mediated metabolism of warfarin, the primary route of warfarin clearance. When CYP2C9 is inhibited, warfarin plasma levels rise and anticoagulant effect intensifies. The consequence is elevated bleeding risk, including intracranial hemorrhage. Direct oral anticoagulants (DOACs) including rivaroxaban and apixaban are metabolized through CYP3A4 and P-glycoprotein pathways, both of which berberine inhibits. Any patient on anticoagulation therapy who takes berberine without physician oversight is accepting an unquantified and potentially serious bleeding risk.
Immunosuppressants. Cyclosporine and tacrolimus, the cornerstone immunosuppressants used after organ transplantation, have narrow therapeutic windows and are metabolized through CYP3A4. Berberine’s CYP3A4 inhibition raises their plasma concentrations, increasing the risk of nephrotoxicity and other dose-dependent toxicities.
Psychiatric medications. A large proportion of antidepressants and antipsychotics, including fluoxetine, paroxetine, haloperidol, risperidone, and aripiprazole, are metabolized primarily through CYP2D6. Berberine’s potent CYP2D6 inhibition raises their plasma concentrations in ways that cannot be predicted without therapeutic drug monitoring. The consequences range from intensified side effects and cardiac arrhythmia.
Antiarrhythmics and beta-blockers. Metoprolol, carvedilol, propafenone, and flecainide are among the cardiac medications metabolized through CYP2D6. Concentration increases in this drug class carry direct cardiac risk, particularly in patients with underlying structural heart disease.
Statins. Several statins, including simvastatin and atorvastatin, are metabolized through CYP3A4. Berberine’s CYP3A4 inhibition raises statin concentrations and increases the risk of statin-associated myopathy and, at high concentrations, rhabdomyolysis.
Insulin and insulin secretagogues. Berberine’s own glucose-lowering effect, combined with the blood-glucose-lowering effect of insulin or sulfonylureas, creates additive hypoglycemic risk. A patient on a sulfonylurea who adds berberine without dose adjustment is at increased risk for hypoglycemic episodes.
The interaction profile is additive. A patient on warfarin, a statin, metoprolol, and an antidepressant, a combination that describes millions of Americans with metabolic and cardiovascular disease, who adds berberine faces simultaneous inhibition of the clearance pathways for all four medications. The cumulative pharmacokinetic effect is not predictable without clinical monitoring (International Journal of Molecular Sciences, 2025;26(11):5188).
A Hard Contraindication
Any pregnant person, or anyone who may become pregnant, should not take berberine. Any breastfeeding person should not take berberine. This applies to berberine from any source, including traditional herbal preparations that contain it.
Berberine displaces bilirubin from albumin, the protein that normally keeps unbound bilirubin in check (Chan E., Biological Neonate, 1993). Chronic administration produces persistent elevation of unbound serum bilirubin in animal models. Berberine crosses the placenta, the neonatal liver lacks the enzymatic maturity to conjugate bilirubin efficiently, making the fetus and neonate specifically vulnerable to bilirubin-induced neurological damage. Case reports associate berberine-containing herbal preparations with neonatal jaundice and kernicterus risk. Berberine also has documented uterotonic properties.
Hepatotoxicity
Isolated case reports associate berberine use with hepatotoxicity. Causality is difficult to establish from case reports, and the evidence base here is limited. This is important for patients with pre-existing hepatic disease.
Who Should Not Take Berberine Without Physician Review
The following people are not candidates for self-directed berberine supplementation. If you are in any of these categories and are considering berberine, that decision requires a conversation with your physician before any purchase.
Anyone taking warfarin or any anticoagulant
Anyone on immunosuppressants following organ transplantation
Anyone taking insulin or any insulin secretagogue, including sulfonylureas
Anyone on antidepressants or antipsychotic medications, particularly those metabolized by CYP2D6
Anyone taking antiarrhythmics or beta-blockers
Anyone with renal impairment
Anyone with hepatic insufficiency or active liver disease
Anyone who is pregnant, breastfeeding, or may become pregnant
Anyone taking any medication with a narrow therapeutic window
Anyone on multiple medications simultaneously, because the interaction profile is additive and unpredictable
This list describes a substantial proportion of the American adults who are most likely to be interested in berberine based on its marketed metabolic indications.
What Should You Take From This Article
First. This piece makes no recommendation for berberine use in any indication. The evidence for glucose lowering and lipid modulation is real, but it comes from selected populations under specific conditions and does not generalize to the broad metabolic wellness market where berberine is primarily sold. The drug interaction profile documented above is a genuine public health concern. Whether berberine’s potential benefits outweigh its risks in any individual patient is a clinical question that requires physician involvement, not a decision made in the supplement aisle.
Second. Almost all of berberine’s cancer-related marketing claims lack human clinical evidence and are implausible at standard oral doses. It is the central pharmacokinetic fact that makes systemic cancer claims incoherent. The one narrow exception where credible clinical evidence exists is colorectal adenoma chemoprevention in post-polypectomy patients, where high luminal concentrations act directly on colonic mucosa and where a well-designed RCT with six-year follow-up data demonstrates durable protective effect (Tan et al., Lancet Regional Health, Western Pacific, 2025). This is not an endorsement, any decision in that specific area belongs with the treating physician.
Third. If you are considering berberine for any reason, the first step is a conversation with your physician about all current medications. Given the drug interaction profile documented in this piece, that conversation is the minimum responsible precaution.
The “natural equals safe” equation is one of the most consequential errors in contemporary health culture. Berberine is a biologically active compound with real pharmacological effects and real pharmacological risks. Biological activity and safety are not the same thing.
Berberine deserves honest evaluation: neither dismissing it because it comes from a plant nor endorsing it because wellness marketing. The science supports specific benefits, but the risks are a real concern.
Found this article useful? Share your thoughts. Join the conversation below.
Educational content on The Metabolic Archives is free, because medical information should be accessible to everyone. If you find value and want to support the work, a paid subscription is available and genuinely appreciated. Visit the About Page for additional information.
The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.