
Beyond Weight Loss: New Research Links Gut Bacteria to Diabetes Remission After Bariatric Surgery
A new study finds that changes in the gut microbiome after bariatric surgery are associated with type 2 diabetes remission

Bariatric surgery is the most effective treatment available for obesity and type 2 diabetes (T2D). But it has always carried an uncomfortable mystery: outcomes are inconsistent.
A study published in Nature Metabolism in May 2026 offers the most rigorous human evidence to date that the gut microbiome the vast community of bacteria living in your digestive tract is part of the answer (Olsson et al., Nature Metabolism 8, 1212–1228, 2026).
Two Different Surgeries
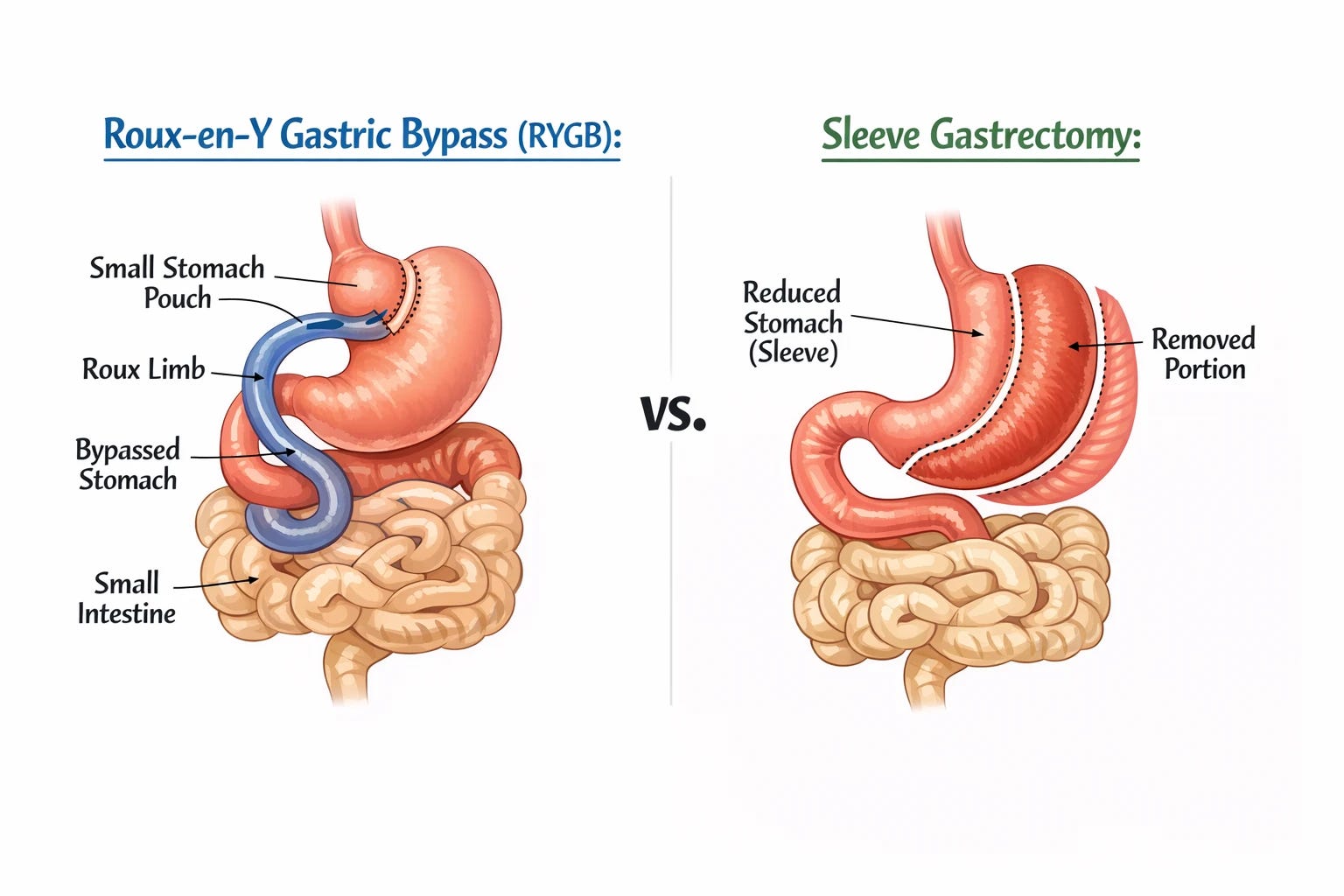
To understand the findings, it helps to know that the two most common bariatric procedures are anatomically quite different.
Roux-en-Y gastric bypass (RYGB) is a major rearrangement of the digestive tract. The stomach is divided into a small pouch, and the small intestine is rerouted so that food bypasses most of the stomach and the upper portion of the small intestine entirely. Sleeve gastrectomy (SG) is a simpler procedure: roughly 80% of the stomach is removed, leaving a narrow tube, but the intestines remain anatomically intact.
The Oseberg Study
The Olsson et al. study is a subanalysis of the Oseberg randomized controlled trial (RCT), conducted in Norway. Seventy-seven patients with obesity and T2D were randomized to either RYGB or SG. Before surgery and again at 12 months, researchers collected stool samples and analyzed the gut microbiome using whole-genome sequencing, which reads the genetic material of the entire microbial community rather than sampling a subset of species. Five-year remission outcome data were also available for analysis.
At 12 months, T2D remission rates were 74% for RYGB versus 52% for SG, a statistically significant difference (logistic regression, P=0.046). RYGB also produced greater weight loss, larger reductions in fasting blood glucose, and stronger post-meal glucagon-like peptide 1 (GLP-1) responses.
RYGB produced larger and more consistent shifts in gut microbial composition across patients accounting for 5.3% of gut microbiota compositional variation, compared with 1.9% for SG. The more extensive anatomical rearrangement of RYGB appears to produce a more forceful, uniform remodeling of the gut microbial environment.
What Remission Looks Like in the Microbiome
Patients who achieved T2D remission showed a distinct microbial profile compared to those who did not.
Remitters had significantly greater increases in bacterial gene richness: a measure of the diversity and functional capacity of the microbial community. Higher gene richness has been linked to better metabolic health in previous research, and in this study the effect of remission status on gene richness increase was larger than the effect of surgery type. The specific bacteria most strongly associated with remission included Alistipes species, Lachnospira eligens, and uncharacterized members of the Christensenellales order.
Butyrate is a beneficial compound produced when gut bacteria break down certain dietary fibers and amino acids. It supports insulin secretion, reduces intestinal inflammation, and helps regulate gut hormone release. A specific gene, ato, which encodes a key step in the lysine-to-butyrate conversion pathway, increased in abundance after surgery exclusively in patients who achieved remission and this was true across both surgery types, independent of how much weight was lost.
The Weight-Independence Finding
The microbiome changes associated with remission were not simply a reflection of losing more weight. After statistical adjustment for degree of weight loss, the association between microbial shifts and remission remained significant (R²=0.03, P=0.001 for surgery type effect after weight-loss adjustment).
Weight loss clearly contributes to T2D remission after bariatric surgery. What this study adds is evidence that the gut microbiome appears to contribute through separate, additional mechanisms. Patients with favorable microbiome shifts also showed better GLP-1 responses and improved beta-cell glucose sensitivity, suggesting a microbiome-to-incretin axis that operates alongside the metabolic effects of weight reduction.
SG produces more variable microbiome shifts between individuals than RYGB does, it creates a natural range of microbial outcomes to examine. In SG patients, the magnitude of microbiome change correlated positively with GLP-1 levels, beta-cell function, and 5-year remission status offering a cleaner window into the relationship between microbial shift and metabolic outcome than the more uniform RYGB response allows.
A Counterintuitive Finding About Butyrate Levels
Despite the increased bacterial capacity to produce butyrate and other short-chain fatty acids (SCFAs) after surgery, measured fecal concentrations of these compounds actually decreased at 12 months. The decrease in propionate and butyrate was driven specifically by the remission group.
The authors’ interpretation: the gut is not producing less butyrate, it is absorbing and using it more efficiently. Think of it this way: if a factory’s output is rising but the warehouse is consistently empty, the goods are being shipped out and used as fast as they are made. Whether that interpretation is correct requires dedicated flux studies. For now, the finding stands as a plausible hypothesis, not an established mechanism.
Could the Microbiome Predict Who Benefits?
A machine-learning analysis using pre-surgical microbiome data found that baseline abundances of Lachnospira eligens, Alistipes senegalensis, Christensenella minuta, and butyrate production genes (ato, 4hbt, buk) were predictive of 5-year T2D remission status. This raises an intriguing possibility: that microbiome profiling before surgery could eventually identify patients most likely to achieve durable remission and guide clinical decision-making.
The modeling was performed on a small sample using XGBoost, a machine-learning method that requires prospective validation in much larger cohorts before any clinical application could be considered. The bacteria identified are not yet fully characterized, and several are not yet reliably isolatable in the laboratory. The authors are appropriately cautious, describing them as candidates for future study rather than therapeutic targets.
Prior Evidence and the Causal Question
This study adds to a growing body of evidence. A 2022 study by Debédat et al. in Gut Microbes followed 100 RYGB patients for five years and found that unresolved T2D was associated with pre-surgical enrichment in specific Bacteroidia species, including Bacteroides fragilis and Phocaeicola dorei (Debédat et al., Gut Microbes 14(1):2050635, 2022). Critically, when stool from poor-outcome human donors was transplanted into germ-free mice, the animals developed impaired glucose tolerance and insulin resistance independent of body weight raising the possibility that the microbiome differences are not just correlating with poor outcomes but contributing to them.
Cross-species translation from mouse models to humans is not straightforward, and the mechanism by which the transplanted microbiome impaired glucose tolerance was not established. The Olsson et al. study does not resolve the causal question in humans all microbiome-remission associations in this paper are correlational.
Limitations
The sample is small: 77 patients across two surgical groups. Metformin use could not be controlled for because it covaried too strongly with remission status in this cohort. Metformin has well-documented independent effects on gut microbial composition, making it impossible to fully separate the surgery’s microbiome effects from the drug’s. Individual effect sizes for microbiome parameters were modest, and the causal chain from microbial shift to metabolic improvement has not been established in humans.
None of these limitations undermine the value of the findings. An RCT design with whole-genome microbiome sequencing, weight-loss-adjusted analysis, and five-year clinical follow-up is a methodological standard that previous work in this area has rarely reached.
What It Means
Bariatric surgery does not work by restricting calories alone. The gut microbial community is being remodeled by these procedures, and that remodeling appears to contribute to whether a patient achieves diabetes remission through mechanisms that extend beyond weight loss. The specific bacteria and metabolic pathways identified here are now candidate targets for microbiome-based interventions: therapeutic probiotics, dietary strategies, or other approaches that might one day replicate or enhance the metabolic benefits of surgery without the surgery itself.
Found this article useful? Share your thoughts. Join the conversation below.
Educational content on The Metabolic Archives is free, because medical information should be accessible to everyone. If you find value and want to support the work, a paid subscription is available and genuinely appreciated. Visit the About Page for additional information.
The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.
Tags: bariatric surgery, gut microbiome, type 2 diabetes, diabetes remission, metabolic health, obesity medicine, short-chain fatty acids, science news