
From Protector to Villain: The Shifting Science of Alcohol
Separating the Evidence from the Mythology

The official guidance regarding social alcohol use has shifted substantially over the past few years, and the shift was never adequately explained to the public. Credible medical sources told you that a daily glass of wine was good for your heart. Now other credible sources tell you that no amount of alcohol is safe. This piece covers what current science means for someone who drinks socially.

Why the Guidance Changed
For most of the 1980s and 1990s, large observational studies consistently found that moderate drinkers had lower rates of cardiovascular disease than non-drinkers. When researchers plotted the relationship between alcohol consumption and heart disease risk on a graph, the curve bent downward at low doses before rising steeply at high doses. The cardioprotective effect of moderate drinking became one of the most cited findings in nutritional epidemiology, and it gave scientific credibility to what many people already wanted to believe: that the glass of wine at dinner was not just pleasurable but beneficial.
Observational studies measure what people do and what happens to them over time. That limitation left the moderate-drinker group quietly contaminated by two systematic errors that made abstainers look sicker than they actually were.
Sick quitter bias: many people who appear in the abstainer category of these studies are not lifetime non-drinkers, they are former drinkers who stopped because of illness.
Healthy user bias: in wealthy Western populations, moderate drinkers tend to cluster with other health-protective behaviors: regular exercise, higher income, better access to healthcare, lower rates of smoking. These factors independently reduce cardiovascular risk.
A 2024 review of 95 cohort studies on alcohol and cardiovascular disease found that the sick quitter problem was the most serious methodological weakness in this literature, identified in the majority of studies reviewed but addressed with highly variable rigor. More telling are the results from Mendelian randomization studies, a methodological approach that uses inherited genetic variants affecting alcohol metabolism as a natural experiment to estimate the effect of consumption without the behavioral confounding that plagues observational research. A 2024 nested case-control study in more than 250,000 participants from the Million Veteran Program, using both observational and Mendelian randomization methods, found that the two approaches produced divergent results: the observationally apparent protective effect for coronary heart disease and type 2 diabetes was not supported by the genetic analysis (Kember et al., Alcohol: Clinical and Experimental Research, 2024).
The Red Wine Carve-Out
The argument runs as follows: wine, particularly red wine, contains resveratrol, a polyphenol compound found in grape skins. Laboratory studies have shown that resveratrol activates certain cellular pathways associated with longevity and metabolic regulation. Therefore, red wine is different from other alcoholic beverages, and its benefits outweigh its harms.

The reality paints a different picture.
Resveratrol is present in red wine, but the concentration is low. A standard glass of red wine contains somewhere between 0.2 and 2 milligrams of resveratrol. The laboratory studies that produced excitement about this compound used doses in the range of hundreds of milligrams per day, applied to cell cultures or animal models. The gap between what a glass of wine delivers and what a study requires to show a biological effect is several orders of magnitude.
The supplement industry responded to this gap by producing purpose-formulated resveratrol capsules at doses far exceeding anything achievable through wine consumption. A 2024 systematic review and meta-analysis of resveratrol supplementation trials found no statistically significant overall effect on glucose metabolism and an increase in triglycerides in some subgroups (Zahoor et al., Obesity Pillars, 2024). A companion 2024 systematic review and meta-analysis examining resveratrol’s effects across metabolic syndrome components reached similarly null conclusions (Endocrines, 2024).
The cellular mechanisms that made resveratrol compelling in the laboratory have not translated into clinical outcomes in humans, even at pharmacological doses that no amount of wine drinking could approach.
The red wine exception also fails on a more basic chemical point. Blood pressure data from a large Danish cohort study, published in the American Journal of Medicine in 2024, found consistent blood pressure effects across wine, beer, and spirits, with no meaningful difference between beverage types (Copenhagen General Population Study, 2024). Ethanol is the same molecule regardless of what surrounds it.
What Alcohol Actually Does
With the cardioprotective claim set aside, the evidence on alcohol’s biological effects points consistently in one direction.
Blood Pressure
A 2024 systematic review and dose-response meta-analysis of 23 cohort studies published in Hypertension found a positive, nearly linear association between alcohol intake and the risk of developing high blood pressure across the full range of consumption, with no evidence of a threshold below which the effect disappears (Cecchini et al., Hypertension, 2024). A companion meta-analysis confirmed the same linear relationship for both systolic and diastolic pressure over time (di Federico et al., Hypertension, 2023).
Cessation data reinforces the causal interpretation. A 2025 longitudinal Japanese cohort study published in the Journal of the American College of Cardiology found dose-dependent blood pressure reductions when participants reduced or stopped drinking, and dose-dependent increases when new drinkers started, with consistent findings across all beverage types.
High blood pressure is a core component of the metabolic syndrome cluster, and alcohol is contributing to it in a dose-responsive fashion starting from the first drink.
If you enjoy evidence-based medical information, subscribe to receive these articles delivered to your mailbox every week.
Visceral Fat and Liver Function
Alcohol provides 7 calories per gram, placing it just below fat in caloric density. Ethanol is preferentially oxidized over both fat and carbohydrates, meaning the body burns it first. While alcohol is being processed, fat oxidation is suppressed, de novo lipogenesis (the conversion of excess energy into fat) is promoted, and insulin signaling is disrupted.
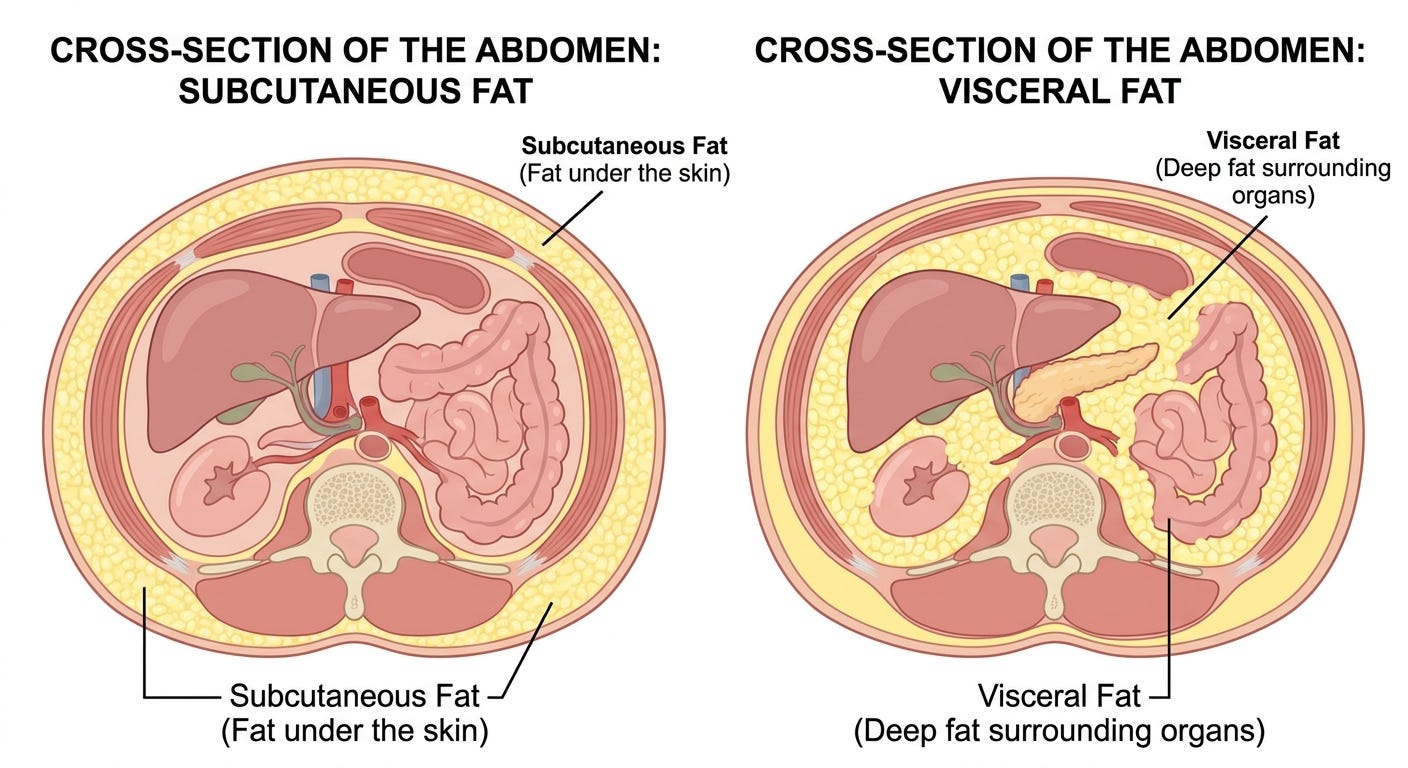
The fat that accumulates as a result is not distributed randomly. An Oxford Biobank study using dual-energy X-ray absorptiometry (DXA) scanning in 5,761 participants found that alcohol consumption increased visceral fat mass in both men and women (International Journal of Obesity, 2022). Visceral fat, the metabolically active fat surrounding the abdominal organs, carries substantially greater cardiometabolic risk than subcutaneous fat.
In patients with pre-existing metabolic dysfunction-associated steatotic liver disease (MASLD), moderate alcohol intake has been found to increase the risk of type 2 diabetes and advanced liver fibrosis, with a synergistic interaction with insulin resistance that accelerates disease progression (Clinical and Molecular Hepatology, 2022). The National Academies of Sciences, Engineering, and Medicine reviewed the available evidence on alcohol and weight-related outcomes in 2025 and reached consistent conclusions about alcohol’s role in promoting visceral adiposity and worsening hepatic disease in vulnerable populations (National Academies Press, 2025).
Sleep Architecture
Alcohol is widely used as a sleep aid and at higher doses it can shorten the time it takes to fall asleep. That is where the benefit ends.
A 2024 systematic review and meta-analysis found that even low-dose alcohol suppresses rapid eye movement (REM) sleep in a dose-dependent fashion, with impairment proportional to consumption across the full range studied (Gardiner et al., Sleep Medicine Reviews, 2024). REM sleep is the stage most closely associated with memory consolidation, emotional regulation, and metabolic recovery. A 2024 study examining consecutive nights of pre-sleep alcohol consumption confirmed cumulative disruption to sleep architecture with repeated use, meaning the problem compounds rather than adapts (McCullar et al., Sleep, 2024).
REM disruption drives the same hormonal cascade that worsens metabolic syndrome independently: cortisol dysregulation, elevation of ghrelin (the hunger-stimulating hormone), and suppression of leptin (the satiety hormone). The nightcap that appears to ease sleep onset is compounding the metabolic burden rather than relieving it.
Gut Microbiome
Is well established that chronic, heavy alcohol consumption is associated with gut dysbiosis, increased intestinal permeability, reduction in beneficial bacterial populations including Lactobacillus species, elevation of pathogenic species, and endotoxemia that drives systemic inflammation and contributes to liver injury (Koutromanos et al., World Journal of Methodology, 2024; Frontiers in Microbiology, 2024). These effects have been documented consistently across multiple research groups and study designs.
For social drinking at lower doses, the data points in same direction but is less certain. Current evidence does not permit a precise threshold statement for this population. The best conclusion for now is that the gut microbiome appears sensitive to alcohol in a dose-dependent fashion, with the clearest findings at higher consumption levels and an emerging but not yet fully quantified picture at moderate intake.
The Cancer Question
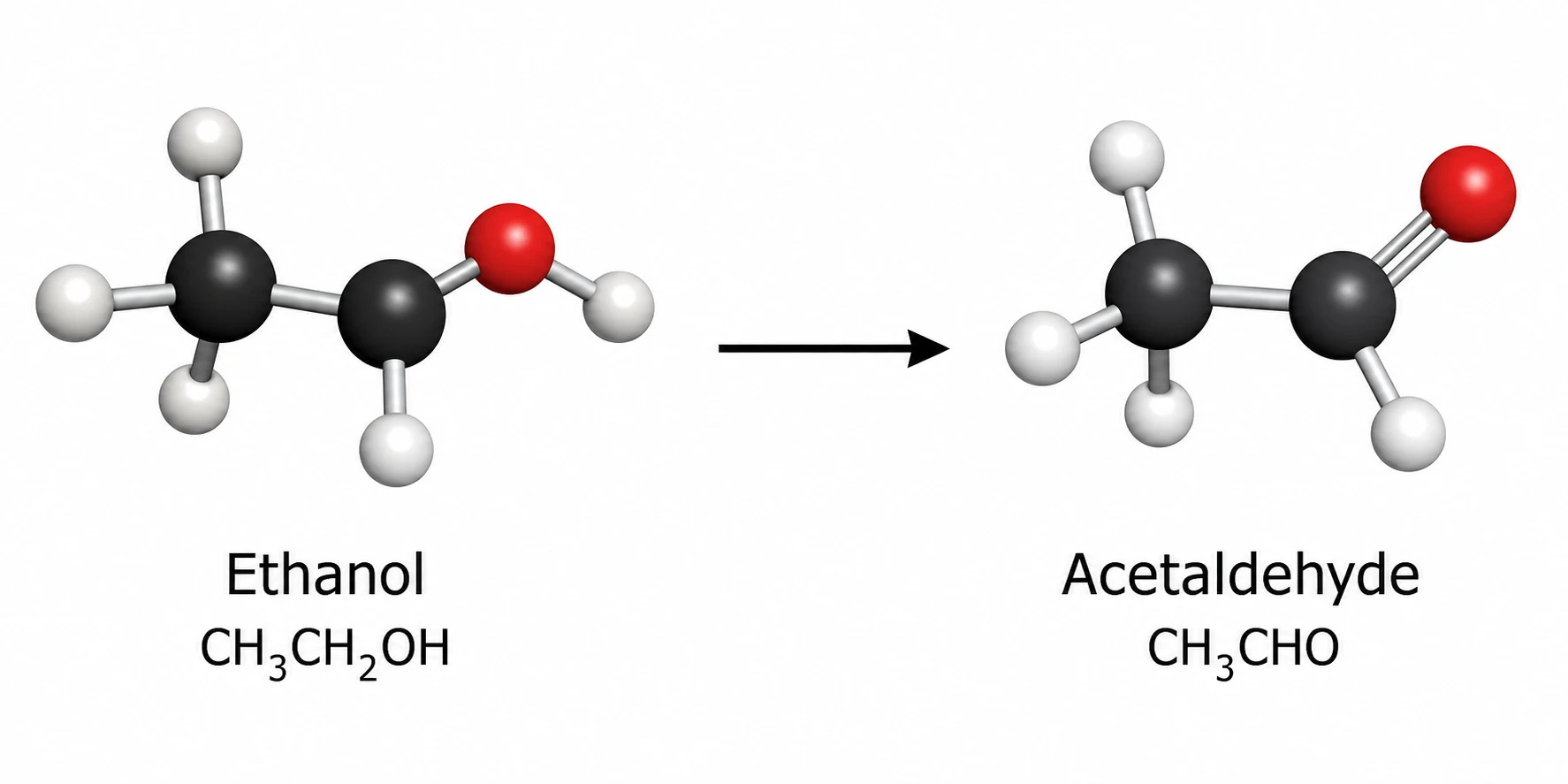
The International Agency for Research on Cancer (IARC) has classified alcoholic beverages as Group 1 carcinogens since 1988. Group 1 means sufficient evidence of causality in humans, the highest classification available. Ethanol and acetaldehyde, its primary metabolite, are each independently classified Group 1. Seven cancer sites are causally linked: oral cavity, pharynx, larynx, esophagus, liver, colorectum, and female breast. The World Health Organization (WHO) reaffirmed in 2023 that no safe threshold for cancer risk can be established and that the dose-response relationship begins at zero (WHO/IARC joint statement, 2023).
The case for causality rests on several lines of evidence. Epidemiological consistency is one: the association between alcohol and these seven cancer sites has been replicated across populations that differ substantially in diet, genetics, healthcare access, and environmental exposures. The cellular mechanism is another. Acetaldehyde, the first breakdown product of ethanol, causes direct damage in the DNA and inhibition of the repair enzymes that would normally correct this damage (Lachenmeier and Salaspuro, Nature Reviews Cancer, 2007; Clinical and Translational Discovery, 2024). Additional mechanisms include induction of the CYP2E1 enzyme generating reactive oxygen species, disruption of DNA methylation patterns, interference with retinoid metabolism, and elevation of circulating estrogen contributing to breast cancer risk.
The most compelling single line of evidence comes from genetics. A common variant in the ALDH2 gene, found predominantly in East Asian populations, impairs the enzyme that clears acetaldehyde after ethanol is metabolized. People carrying this variant who drink accumulate acetaldehyde at substantially higher concentrations than normal metabolizers. Their rates of upper respiratory and digestive tract cancers are dramatically elevated compared to both non-carriers who drink and non-drinkers of any genotype. This natural experiment provides strong support for the acetaldehyde-mediated mechanism because it isolates the variable, acetaldehyde clearance capacity, while holding consumption behavior relatively constant. Cessation data add further weight: stopping drinking reduces the risk of oral and esophageal cancer, with the reduction proportional to duration of abstinence (Freisling et al., IARC Handbooks Working Group, New England Journal of Medicine, 2023).
In evaluating the strict conclusions expressed by these health organizations, in my personal opinion the evidence is not conclusive enough to support them. Let me explain why:
Cancer studies require observation windows measured in years to decades. Over those timescales, study participants are simultaneously exposed to a large and varied landscape of other carcinogens: environmental pollutants, dietary factors, occupational exposures, and the background carcinogenic burden of modern industrial life. Fully accounting for those exposures is genuinely difficult, and in long-duration cancer epidemiology the confounding burden is substantial. The IARC Group 1 classification addresses a specific question: is there sufficient evidence that alcohol causes cancer in humans? The answer to that question is yes. It does not address a separate question: at social drinking levels, in a population already carrying meaningful background carcinogenic exposure from other sources, what is the precise incremental cancer risk attributable to alcohol?
What This Means for You
We can say with confidence that there is no identified dose of alcohol that confers a net health benefit: the cardioprotective story was a methodological artifact, and the resveratrol story was a laboratory finding that never survived clinical testing. What the evidence consistently shows, across blood pressure, visceral fat, liver function, sleep architecture, and cancer biology, is a dose-dependent pattern of harm without a protective floor.
Abstinence is the single best recommendation, if you do not drink there is no reason to start. For those unwilling to adopt abstinence, the evidence clearly supports aggressive reduction of total alcohol intake.
The case for elimination is particularly strong if you are already managing metabolic syndrome, elevated blood pressure, or hepatic steatosis. In each of those conditions, alcohol is synergizing with existing disease processes in ways that compound the risks.
The official position changed because better research tools revealed what earlier tools could not: the protection was never real, and the harm was always present.
Found this article useful? Share your thoughts. Join the conversation below.
The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.