
Lifestyle Modification: The Most Powerful Treatment You Were Never Taught
Part Five: Taking Control of Your Sleep

No single behavioral change transforms sleep by itself. What follows is a scientific exploration of proven strategies to promote and improve sleep. This article leans heavy on science to explain the individual mechanisms that support these interventions, with actionable recommendations in plain language included for you to incorporate into your sleep routines.
Wind-Down Is a Biological Requirement
The 30 to 60 minutes before sleep is the time to wind-down before sleep. The pre-sleep environment is important to support sleep.
The single strongest non-pharmacological pre-sleep intervention with randomized controlled trial support is a warm bath or shower taken approximately 90 minutes before your target sleep time. A 2019 systematic review and meta-analysis by Haghayegh et al. in Sleep Medicine Reviews found a 36% reduction in sleep onset latency with this approach. The mechanism is peripheral vasodilation: warm water draws blood toward the skin, accelerating the drop in core body temperature that the circadian system uses to initiate sleep. The timing of 90 minutes is when the vasodilation effect on core temperature is strongest.
Room temperature works through the same mechanism. Across datasets including an analysis of 3.75 million nights by Rifkin et al. and a 2025 synthesis of 134 studies in Indoor Air, the consistent finding is that cooler sleeping environments improve sleep quality. The evidence suggests 64 to 68 degrees Fahrenheit (18 to 20 degrees Celsius) as optimal. Bedrooms running warmer than 70 degrees Fahrenheit are associated with poorer sleep quality in the Rifkin data.
Lighting in the hour before sleep matters for two reasons: photonic suppression of melatonin and conditioned arousal from screen content. The practical standard for pre-sleep lighting is warm-spectrum illumination below 2700K at low intensity, positioned as indirect or shaded rather than direct task lighting. Television in bed compounds both problems: retinal photon dose, content-driven cognitive arousal, and disruption of the conditioned association between your bed and sleep onset.
On blue light blocking glasses and Night Shift mode: both are appealing in theory and underwhelming in evidence. A 2025 systematic review and meta-analysis of three double-blind crossover RCTs in Frontiers in Neurology (Luna-Rangel et al.) found non-significant effects across all four sleep parameters for commercially available blue light blocking glasses. The Lighting Research Center’s evaluation of Apple’s Night Shift concluded that turning devices off two hours before bed remains the evidence-supported recommendation. Night Shift produces a partial spectral shift insufficient to eliminate melanopsin activation at typical screen brightness; screen brightness contributes as much to the problem as spectral content. Neither technology substitutes for device removal.
For pre-sleep activity in the wind-down window, the evidence favors passive engagement over active. Passive narrative fiction, reduces cognitive arousal without generating sympathetic nervous system activation. Progressive muscle relaxation, discussed in the CBT-I section below, is also effective here. A 2026 meta-analysis of 31 RCTs involving 2,277 participants confirmed measurable sleep quality improvement and anxiety reduction across population groups, and a 2022 PSG study by Simon et al. confirmed that PMR specifically increases slow-wave sleep.
Wake Time Is the Anchor
Consistent scheduling is the behavioral foundation of circadian entrainment. Most people who struggle with sleep focus on bedtime; biology points to wake time.
The suprachiasmatic nucleus (SCN) is primarily entrained by the morning light signal. Homeostatic sleep pressure then accumulates across the waking day, reaching its peak as bedtime approaches. Trying to control bedtime without anchoring wake time works against this sequence.
Fix the wake time first, bedtime follows from it.
Morning light exposure is the most potent daily entraining tool available and requires nothing more than going outside. Outdoor light ranges from 10,000 lux on an overcast day to 100,000 lux in direct sun. Indoor light through a window typically falls below 500 lux. Ten minutes of outdoor exposure in the first hour after waking delivers the phase-advancing signal the SCN requires. For those who cannot go outside regularly, a 10,000 lux light therapy box used in the morning is an effective alternative with robust evidence, particularly relevant for northern latitudes in winter and for people with mobility limitations.
A 2023 meta-analysis by Bouman et al. in the Journal of Sleep Research found that social jet lag, defined as the discrepancy between biological sleep timing on work days versus free days, is independently associated with metabolic syndrome and type 2 diabetes. Sleeping in by 90 minutes or more on Saturday and Sunday initiates a measurable circadian phase delay physiologically equivalent to mild westward jet lag. The fatigue that accumulates by Monday morning is not sleep debt, is circadian misalignment produced by the weekend phase shift. Maintaining wake time within one hour of weekday timing on weekends prevents it.
For those who work shift schedules, a 2025 umbrella review of meta-analyses by Cho et al. in the Journal of Sleep Research compared fixed versus rotating shift work through December 2024. Fixed night shift workers carry higher cardiovascular and obesity risk; rotating shift workers carry higher cancer and pregnancy complication risk, because rotating shift workers never achieve stable entrainment in either direction. Forward rotation (morning to afternoon to night) was substantially better tolerated than backward rotation, with nearly double the odds of poor sleep quality for backward rotation in a study of 4,750 workers. Where shift schedules are unavoidable, consistent timing on days off and forward rotation direction reduce circadian disruption without eliminating it.
Shortened winter photoperiod at higher latitudes produces progressive circadian phase delay in susceptible individuals as the SCN receives insufficient morning light to maintain entrainment. Seasonal affective disorder (SAD) is not simply a mood disorder with seasonal timing, is a circadian disorder in which hypersomnia, carbohydrate craving, weight gain, and profound fatigue are the metabolic manifestations. The carbohydrate craving specifically runs through serotonin: reduced winter sunlight decreases serotonin synthesis, and carbohydrate consumption transiently increases brain serotonin availability through insulin-mediated tryptophan uptake. Morning light therapy is the first-line treatment and works through the identical mechanism as the morning light recommendation above.
The circadian clock shifts at approximately one to two hours per day under optimal entraining conditions. Full re-entrainment following significant disruption requires days to weeks. A 2024 study in Sleep on simulated night-shift work found incomplete circadian adjustment even after 96 hours under controlled conditions. Accurate expectations prevent premature abandonment of an intervention that is working.
Exercise As Sleep Intervention
A 2025 network meta-analysis of 86 RCTs involving 7,276 participants published in BMC Public Health found that combined aerobic and resistance training produced the strongest sleep quality improvements of any exercise modality examined. A separate 2025 comparative efficacy analysis of 18 studies involving 1,214 adults found exercise interventions improved sleep efficiency by a mean of 2.85%, reduced wake after sleep onset by an average of 10 minutes, and extended slow-wave sleep by an average of 2.19 minutes on polysomnography (PSG).
For aerobic exercise specifically, a 2025 meta-analysis by Rubio-Valles and Ramos-Jimenez found moderate-intensity aerobic exercise reduced sleep onset latency by 55%, reduced wake time by 30%, and increased total sleep time by 18%, with a 13% improvement in sleep efficiency. The anti-inflammatory mechanism is direct: aerobic exercise reduces IL-6 and TNF-alpha, connecting the intervention explicitly to systemic inflammation. The optimal dose from the 2025 network meta-analysis is three sessions per week of 45 to 60 minutes at moderate intensity for 8 to 12 weeks.
Resistance training contributes through a different but complementary mechanism. The Souza et al. 2022 RCT using PSG in sarcopenic older adults (IJERPH, PMC9736460) reduced sleep onset latency from 30 to 16 minutes and increased N3 percentage. The mechanism involves growth hormone secretion during recovery, which is concentrated in slow-wave sleep. Combined aerobic and resistance training consistently outperforms either modality alone across the network meta-analysis literature.
Scheduled exercise at consistent times shifts melatonin onset timing and reinforces circadian alignment through core body temperature changes, adrenergic activation, and neuroendocrine output. Morning exercise specifically lowers post-waking cortisol and produces sustained circadian reinforcement across the day.
A real-world analysis of 150,000 nights (PMC8599432) found no meaningful association between evening physical activity and sleep quality in free-living adults. A 2025 Nature Communications analysis of 4,084,354 person-nights established the practical threshold: exercise bouts ending four or more hours before sleep onset are not associated with any sleep impairment regardless of intensity. Within that four-hour window, higher intensity produces more disruption than moderate intensity. Vigorous exercise ending within one hour of bedtime impairs sleep onset latency, total sleep time, and efficiency across multiple studies.
The hierarchy in plain terms: morning exercise is optimal. Evening moderate-intensity exercise ending more than two hours before bed produces no meaningful disruption. Evening vigorous exercise more than four hours before bed is safe. Evening vigorous exercise within one hour of bed causes modest, acute disruption. Exercise at any realistic time is vastly superior to no exercise for both sleep quality and metabolic health.
If you enjoy evidence-based medical information, subscribe to receive these articles delivered to your mailbox every week.
The Most Effective Insomnia Treatments
Cognitive behavioral therapy for insomnia (CBT-I ) is the gold-standard first-line treatment for chronic insomnia according to the American Academy of Sleep Medicine, the American College of Physicians, and the European Sleep Research Society.
A component network meta-analysis by Furukawa et al. published in JAMA Psychiatry in 2024, encompassing 241 trials and 31,452 participants, identified the active ingredients: cognitive restructuring (incremental OR for remission 1.68), third-wave components (iOR 1.49), sleep restriction (iOR 1.49), and stimulus control (iOR 1.43). Sleep hygiene education alone was not essential (iOR 1.01). A separate 2024 network meta-analysis by Furukawa et al. in Psychiatry and Clinical Neurosciences found CBT-I produced superior long-term remission compared to pharmacotherapy. A 2023 systematic review (PMC10244489) confirmed CBT-I reduces HbA1c and CRP compared to controls, connecting the behavioral intervention directly to metabolic outcomes.
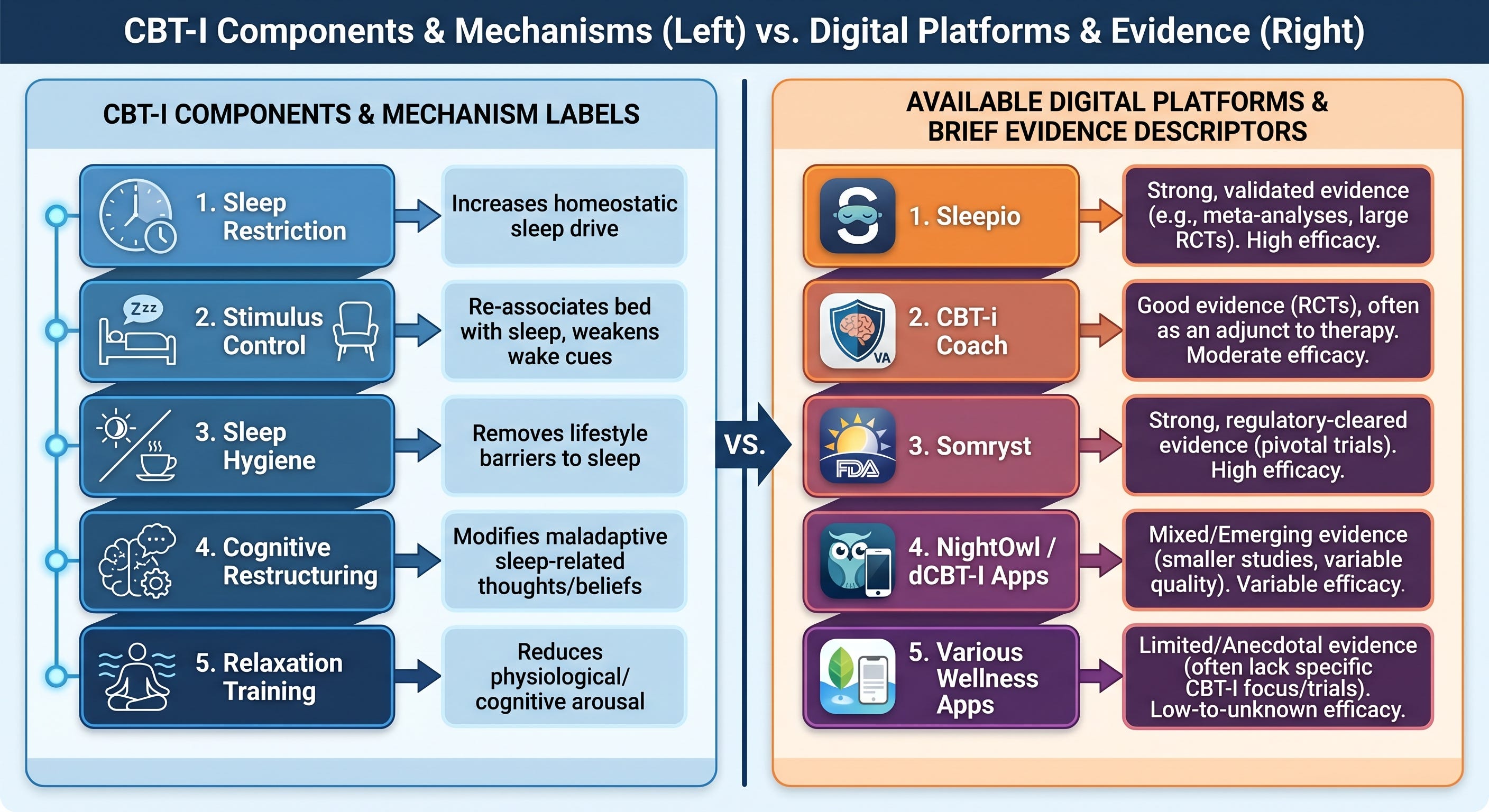
Stimulus control rebuilds the conditioned association between bed and sleep. The rules: bed only for sleep and sex; leave bed after approximately 20 minutes of wakefulness at night and return only when sleepy; consistent wake time regardless of the previous night’s sleep duration; no daytime napping. The mechanism is classical conditioning. The bed becomes a stimulus that reliably predicts sleep, and expectation shapes the physiological response. This is the most foundational component.
Sleep restriction therapy temporarily limits time in bed to actual sleep time, creating controlled sleep pressure that consolidates fragmented sleep and rebuilds efficiency. It is counterintuitive and among the strongest individual components. It is not appropriate for self-administration without guidance in bipolar disorder or seizure disorders, and warrants a conversation with a physician or sleep specialist in those populations.
Cognitive restructuring identifies and challenges automatic negative thoughts about sleep: catastrophic predictions, rigid beliefs about sleep requirements, hypervigilance toward sleep cues. The goal is accurate thinking, not positive thinking. “I cannot function without eight hours” activates pre-sleep cortisol. Examining that thought against actual evidence of prior functioning reduces the activation.
Constructive worry uses a designated 15 to 20 minute period earlier in the evening, at a desk and not in bed, to write down concerns with one concrete next step for each. When worry arises at bedtime, it is acknowledged and deferred. The bed is not the place for problem-solving.
Two relaxation techniques require no equipment, no training, and are available tonight:
The 4-7-8 breathing technique: inhale through the nose for four counts, hold for seven, exhale completely through the mouth for eight. Repeat four cycles. The extended exhale is the active ingredient, activating vagal tone and reducing sympathetic activity. Any ratio where the exhale is twice the inhale length achieves the same mechanism. A 2025 scoping review confirmed increased heart rate variability and decreased systolic blood pressure through parasympathetic activation.
Progressive muscle relaxation: systematic tension and release of muscle groups from feet upward. Five seconds of firm tension per group, ten seconds of complete release, attention directed to the contrast. Ten to 15 minutes for the full sequence. Many people fall asleep before completing it. The 2026 meta-analysis of 31 RCTs and the 2022 PSG study by Simon et al. provide the evidence base.
Behavioral sleep medicine specialists are scarce outside major metropolitan areas. Digital CBT-I resolves the access problem with a robust published evidence base. The 2025 SleepioRx RCT of 336 US adults with DSM-5 insomnia disorder found statistically and clinically significant improvements in insomnia severity at 10 weeks (Cohen’s d = 0.60), strengthening at 16 weeks (d = 0.65) and 24 weeks (d = 0.77). A 2023 PSG RCT of an online CBT-I program (Eigl et al., Clocks Sleep, PMC10594462) confirmed reduced wake after sleep onset from 58.6 to 42.5 minutes and improved sleep efficiency from 86.0% to 89.2% on objective measurement. Available platforms with published evidence: Sleepio (strongest published evidence base), CBTI Coach (free, developed by the VA, available on iOS and Android), and SleepioRx (FDA-regulated, available through healthcare providers). In-person CBT-I with a trained therapist remains the gold standard. Digital CBT-I is a genuine and effective intervention, not a compromise.
Melatonin, Not a Sleeping Pill
Melatonin is a hormone that signals the timing of darkness to the suprachiasmatic nucleus. Its primary biological role is circadian phase shifting, not sedation. It does not induce sleep the way a sedative does. It repositions the internal clock relative to the external light-dark cycle.
Its clearest evidence-supported application is jet lag. The Cochrane review by Herxheimer et al. (PMC8958662) confirmed effectiveness for preventing and reducing jet lag across five or more time zones, with the strongest effects for eastward travel. Taken at the destination’s local bedtime on arrival day, melatonin initiates a phase advance, shifting the internal clock toward the new time zone faster than light exposure alone. Timing relative to the internal clock’s current phase determines the direction of effect entirely: evening administration produces a phase advance, morning administration produces a phase delay. The same mechanism applies to social jet lag and schedule disruption recovery, at lower magnitude.
A secondary and real effect is modest reduction in sleep onset latency, documented consistently across the meta-analysis literature and produced without disrupting sleep architecture.
The dose problem is worth understanding directly. Commercial supplements typically contain 5 to 10 mg. Endogenous nocturnal melatonin peaks at approximately 100 to 200 picograms per milliliter, a concentration that 0.3 to 0.5 mg of exogenous melatonin approximates. A 5 mg dose produces blood levels 10 to 30 times the physiological nocturnal peak. At the receptor level, MT1 and MT2 affinity is calibrated to physiological concentrations: the pKi values for human melatonin receptors indicate half-saturation well below 1 nM, meaning supraphysiological doses saturate and desensitize receptors rather than producing proportionally greater effects (Reiter et al., PMC8006026). A 2024 dose-response meta-analysis by Cruz-Sanabria et al. in the Journal of Pineal Research, evaluating 26 RCTs and 1,689 observations, found that administration timing matters as much as dose in determining efficacy, with effects on sleep onset latency and total sleep time optimized when melatonin is taken two to three hours before the target sleep time rather than 30 minutes. The morning grogginess experienced by many current users of 5 to 10 mg tablets is the predictable consequence of supraphysiological dosing and its persistence into the morning phase-delay zone. Reducing to 0.5 mg and shifting administration to 90 minutes before bed resolves this in most cases.
Melatonin is not FDA-approved for any indication in the United States. It is a dietary supplement not subject to pharmaceutical manufacturing standards. Independent testing has found substantial discrepancies between labeled and actual content. Third-party certification (USP or NSF) reduces but does not eliminate labeling accuracy risk.
About White Noise
A white noise machine or a free app set to low volume is an inexpensive, immediately available tool with real evidence behind it. A 2025 systematic review and meta-analysis of 12 controlled trials involving 1,301 participants published in Sleep confirmed that white noise improves sleep efficiency and reduces nighttime awakenings, with the strongest benefits in noisy environments.
A simpler and equally effective variation requires nothing more than a pair of soft silicone earplugs. By sealing the ear canal, they amplify the sound of your own breathing into a steady, rhythmic background, a self-generated masking sound that crowds out both external noise and the mental chatter that delays sleep onset. Soft silicone earplugs are preferable to foam for overnight use: they conform to the ear canal without the sustained pressure that makes foam uncomfortable after a few hours.
Sedation Is Not Sleep
Every medication below produces sedation, but none produces sleep in the biological sense, with its staged architecture of NREM and REM cycling, slow-wave consolidation, and glymphatic clearance. The question is what it does to the sleep you have while unconscious.
A phenomenon experienced by most people using sleep aids chronically is reduced efficacy overtime: this is secondary to two mechanisms, tachyphylaxis and tolerance. Tachyphylaxis is rapid reduction in receptor-level response following repeated administration, through acute desensitization, receptor internalization, or uncoupling of signaling. Tolerance is broader: receptor downregulation, altered neurotransmitter synthesis, and compensatory upregulation of opposing pathways. Remove the drug and the excitatory upregulation is unopposed, producing rebound insomnia and anxiety that are frequently worse than the original complaint. Any sleep medication is not for continued use, but only for occasional use when needed.
Benzodiazepines enhance GABA-A receptor activity, reducing sleep onset latency and nocturnal awakenings in the short term. The PSG consequences work directly against the architecture of restorative sleep: increased N2, decreased N3 slow-wave sleep, and dose-dependent REM reduction. A 2024 review by Jupe et al. in European Psychiatry (PMC11862261) and a 2025 PSG study by Barbaux et al. in Sleep confirmed both the architectural disruption and the suppression of slow oscillation and spindle coupling that underlies memory consolidation. Long-term consequences include a 65% higher risk for dementia in a 2025 Canadian case-control study (Journal of the Neurological Sciences), doubled risk with long half-life agents, and documented cognitive decline across multiple domains. A 2023 US survey of 1,207 benzodiazepine users found 76.6% reported discontinuation symptoms persisting one year or longer. Benzodiazepines are indicated for two to four weeks maximum in acute situational insomnia. They are contraindicated for chronic insomnia management.
Z-drugs (zolpidem and related agents) act on the same GABA-A receptor complex with greater alpha-1 subunit selectivity, introduced as architecturally superior to benzodiazepines. The 2025 PSG study by Barbaux et al. confirmed that chronic Z-drug use disrupts slow oscillations and spindle coupling comparably to benzodiazepines. Tachyphylaxis and rebound insomnia on discontinuation are documented. The American Geriatrics Society Beers Criteria lists Z-drugs as medications to avoid in older adults due to fall risk, cognitive impairment, and motor vehicle accident risk. Indicated: short-term acute situational use with explicit duration limits.
Trazodone at 25 to 100 mg is among the most commonly prescribed sleep medications in the United States despite no FDA approval for insomnia. The 2022 PSG meta-analysis by Zheng et al. in Scientific Reports (PMC9402537), encompassing 11 RCTs, found trazodone reduces sleep onset latency, reduces wake after sleep onset, increases total sleep time, increases N3 slow-wave sleep, and improves sleep efficiency. The N3 finding is architecturally favorable, the opposite of benzodiazepines. No dependence liability comparable to GABAergic agents. The evidence base is smaller and weaker than approved sleep medications, no long-term controlled insomnia trials exist, and adverse effects include orthostatic hypotension with fall risk in older adults, morning sedation, priapism at higher doses, and cardiac conduction effects. A 2024 CNS Drugs systematic review concluded the adverse effect profile requires careful individual risk-benefit assessment.
Low-dose doxepin at 3 to 6 mg is FDA-approved specifically for sleep maintenance insomnia, functioning through selective histamine H1 receptor antagonism at these doses, a fundamentally different pharmacological profile from antidepressant doses. It improves sleep maintenance, reduces wake after sleep onset, and carries a safety profile comparable to placebo in clinical trials. No dependence liability. The architectural cost is REM reduction. In older adults, anticholinergic effects become relevant even at low doses given reduced cholinergic reserve with aging.
Orexin receptor antagonists (DORAs) are the most architecturally favorable pharmacological option currently available. Suvorexant, lemborexant, and daridorexant are FDA-approved. The mechanism is selective blockade of orexin neuropeptide signaling at OX1R and OX2R removes the drive to wakefulness rather than imposing sedation. A 2025 MDPI International Journal of Molecular Sciences review (PMC12429101) confirmed DORAs facilitate sleep onset and maintenance without disrupting natural sleep architecture. Suvorexant increases both REM and NREM sleep. A network meta-analysis of 20 medications for primary insomnia (Yue et al., Sleep Medicine Reviews, 2023) found DORAs had the highest values across all sleep parameters with the second-best safety profile behind placebo. In the SUNRISE 1 Phase 3 trial, lemborexant demonstrated superior efficacy to zolpidem extended-release with better next-morning cognitive and psychomotor performance. A 2023 RCT by Lucey et al. in Annals of Neurology found acute suvorexant reduced CSF amyloid-beta and phosphorylated tau. That finding requires longer-term replication before clinical interpretation. Tolerance and rebound profiles are more favorable than GABAergic agents. Practical access barriers: DORAs are Schedule IV controlled substances and substantially more expensive than generic alternatives.
No pharmacological agent replaces CBT-I for chronic insomnia. Medications address the symptom. CBT-I addresses the mechanism. The appropriate use of pharmacotherapy is short-term bridging while behavioral treatment is being established, or adjunctive support when behavioral intervention alone is insufficient. Any medication change or discontinuation should be managed with your physician.
Where to Begin
Sleep quality is cumulative. The degree of benefit is proportional to the degree of implementation, and implementation does not require reorganization of your life.
The behavioral interventions are the foundation. Melatonin, used correctly at physiological doses and appropriate timing, is a targeted tool for specific circadian applications, not a nightly supplement. Pharmacotherapy, when genuinely indicated, is a short-term bridge while behavioral treatment is established.
Every tool in this piece is available to you immediately. No prescription is required for the behavioral interventions. No specialist appointment is required to begin CBT-I via CBTI Coach tonight, free of charge, on your phone. Start with the change most accessible to your current life and build from there.
Sleep is not something that happens to you. It is something you can learn to protect.
Found this article useful? Share your thoughts. Join the conversation below.
Educational content on The Metabolic Archives is free, because medical information should be accessible to everyone. If you find value and want to support the work, a paid subscription is available and genuinely appreciated. Visit the About Page for additional information.
The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.