
Obesity: More Than Just A Weight Problem
Why Obesity is Both a Symptom, and a Disease — Part 2


Part 1 of this series laid out what obesity is and what drives it: from ultra-processed food environments to chronic stress, sleep deprivation, psychiatric factors, family conditioning, cultural food traditions, and the structural realities of the built environment.
This post takes you inside your body to show you what obesity is actually doing once it is established and more importantly, what you can do about it at every stage.
Your Body Has a Thermostat
Your body has a sophisticated biological system designed to keep energy balance stable without requiring conscious effort from you. Think of it as the thermostat that monitors incoming and outgoing energy and makes continuous adjustments to maintain equilibrium. This system works through a coordinated cast of hormones each playing a specific role:
Ghrelin is produced primarily in the stomach and signals hunger to the brain. It rises before meals and falls after eating.
Leptin is produced by fat cells and signals fullness and energy sufficiency. When fat stores are adequate, leptin tells the brain to reduce appetite and increase energy expenditure.
GLP-1 and PYY are released from the gut after meals and reinforce satiety, slowing gastric emptying and reducing the drive to keep eating.
Insulin, produced by the pancreas, manages blood glucose by facilitating uptake into cells. It exerts additional metabolic effects through other mechanisms.
Cortisol, the primary stress hormone, mediates the body’s response to threat and affects appetite, fat distribution, and metabolism.
Dopamine drives the brain’s reward and craving circuitry, making certain foods feel compelling and rewarding (i.e., sweets binging after a breakup).
When this system functions properly, energy balance is largely self-regulating. You eat, satiety signals rise, appetite decreases, you stop. You burn energy, fuel stores deplete, hunger signals rise, you eat again. The thermostat maintains its set point automatically without additional intervention needed.
How the Thermostat Breaks
As visceral fat accumulates it releases excess free fatty acids and pro-inflammatory molecules that travel to the liver, muscle, and pancreas, triggering low-grade systemic inflammation that progressively impairs insulin signaling throughout the body. This mechanism is well-documented in a 2021 adipose tissue review published in ScienceDirect. The fat itself becomes an active participant in disrupting the systems that regulates it.
Leptin resistance develops when the brain loses its ability to respond to the fullness signals accurately. In obesity, leptin levels in the bloodstream are actually elevated, fat cells are producing higher amounts. But obesity impairs leptin’s transport across the blood-brain barrier by reducing the specific molecular transporters that carry it through, according to a 2025 PMC review of leptin resistance mechanisms. The result, as documented in a 2021 paper in Frontiers in Endocrinology, is reduced satiety, continued overconsumption, and progressive weight gain.
Insulin resistance develops as systemic inflammation and visceral fat accumulation impair insulin signaling, and cells throughout the body become less responsive to it. The pancreas compensates by producing more and more insulin. Blood sugar control becomes increasingly impaired. Critically, research published in MDPI Biomedicines in 2025 suggests that adipose tissue insulin resistance often precedes systemic insulin resistance and the clinical diagnosis of diabetes by several years meaning the metabolic cascade is well underway long before standard blood tests would catch it. A 2024 PMC analysis found that visceral fat carries stronger predictive value for adipose tissue insulin resistance than BMI, waist circumference alone, or total body fat percentage; more on that below.
Excess visceral fat degrades the regulatory system. The degraded regulatory system makes it harder to reduce visceral fat. Inflammation and insulin resistance generate their own momentum with the process becoming increasingly self-sustaining.
If you enjoy evidence-based medical information, subscribe to receive these articles delivered to your mailbox every week.
The Four Stages and Where You Want to Be
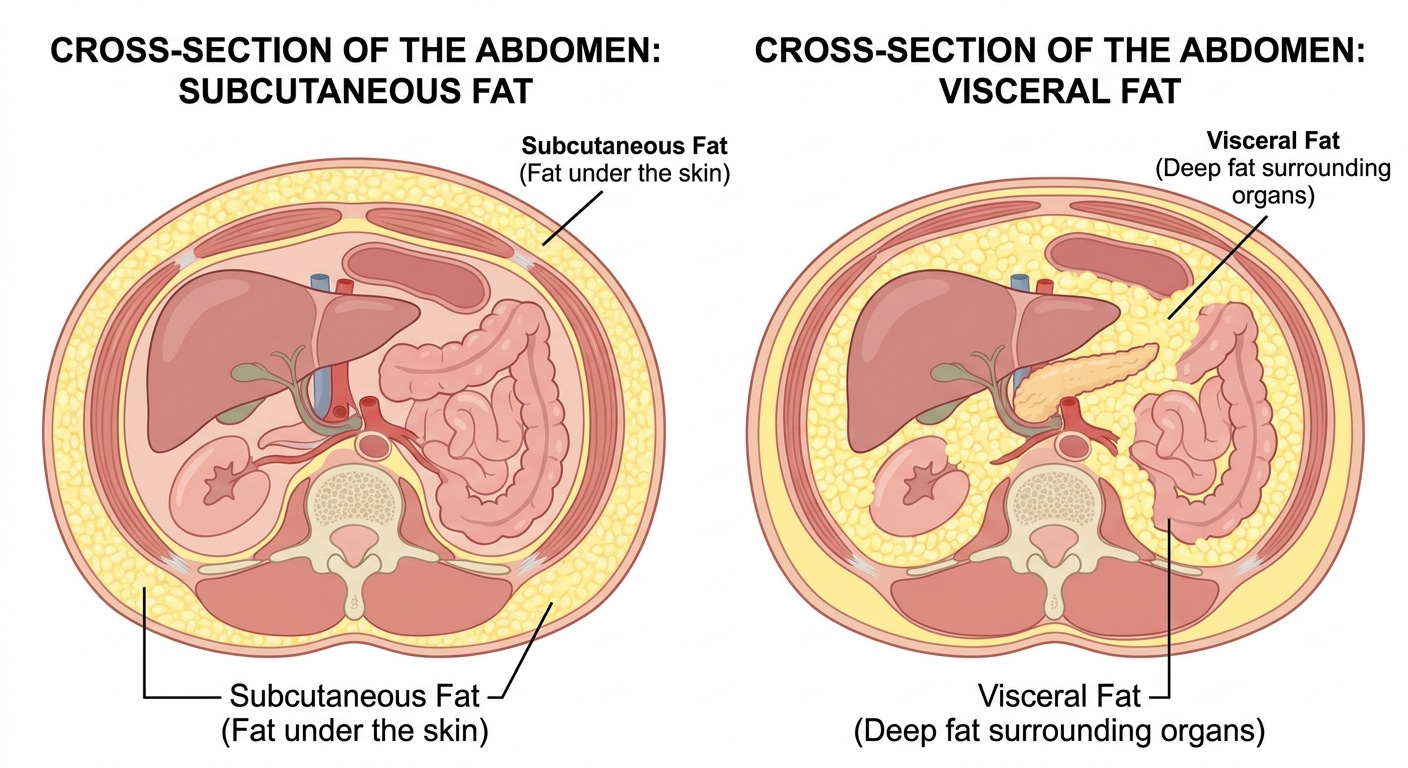
Stage 1: Subcutaneous obesity. Excess fat is accumulating primarily beneath the skin. Metabolic disruption is minimal. The thermostat is functioning, even if energy balance is off. This is the stage where lifestyle intervention has maximum power, before subcutaneous stores become overburden leading to visceral fat accumulation.
Stage 2: Visceral fat accumulation. Fat is deepening into the abdominal cavity, surrounding the organs triggering inflammation. Leptin transport is starting to become impaired. Intervention at this stage is still highly effective but the biology is beginning to work against you rather than with you.
Stage 3: Established insulin resistance. The pancreas is compensating. Blood glucose regulation is impaired. The system is no longer simply dysregulated, it is defending the dysregulation. Intervention here is still meaningful and important, but it requires more sustained effort and often benefits from medical support.
Stage 4: Full metabolic syndrome. A convergence of abdominal obesity, elevated blood glucose, high blood pressure, abnormal lipid levels, and systemic inflammation operating simultaneously. This is where the most serious downstream diseases, type 2 diabetes, cardiovascular disease, fatty liver disease, and others, become immediate rather than distant risks.
Your agency to interrupt this process is greatest at Stage 1 and diminishes progressively across the spectrum.
The concept of “metabolically healthy obesity”, the idea that some people carry significant excess weight without metabolic consequences, is real in the short term and genuinely misleading in the long term. Longitudinal data from the MESA study, published in JACC in 2018, found that a substantial proportion of individuals in the metabolically healthy obesity category transition to metabolic disease over time, at a rate that tracks with cumulative obesity duration and severity.
A Simple Tool You Can Use Right Now

Weight and BMI alone are poor proxies for metabolic risk. The essential point here is simpler: where fat is located matters more than how much you weigh.
The tool that captures this most practically is the waist-to-height ratio. Is a simple screening tool has a good track record for identifying people at increased metabolic risk.
Here is what you can do at home. Find a piece of string. Cut it to your height. Fold it in half. Now try to wrap that folded string around your waist at the level of your navel. If it does not reach, if your waist circumference is greater than half your height, that is a reason to seek additional metabolic evaluation from your doctor as soon as possible.
This assessment costs nothing, requires no equipment beyond a piece of string, and takes about thirty seconds. Research published in PMC in 2024 confirms that visceral fat is the strongest predictor of adipose tissue insulin resistance when compared to BMI, waist circumference alone, and total body fat.
A Word on Dignity and the Cultural Conversation
There is an active public debate about body acceptance, weight stigma, and whether obesity is a health issue or primarily a social one.
Three things are simultaneously true, and none of them cancels the others:
Better public accommodation for people living with obesity is reasonable, practical, and worthy goal. It is just basic dignity.
Weight stigma causes documented and serious harm. According to a 2020 joint international consensus statement in Nature Medicine, stigma is associated with healthcare avoidance, reduced utilization of medical services, worsened eating behavior, lower physical activity, and increased weight gain over time. AAFP data from 2022 indicates that nearly 70% of people with overweight or obesity report feeling stigmatized by physicians and women in particular delay seeking care to avoid weight-related shame. A 2024 review documented fewer cancer screenings and less intensive diabetes management in patients with obesity, showing that stigma causes not just emotional harm, but a concrete clinical one.
The evidence that obesity is health-neutral is not there. The American Heart Association’s 2021 scientific statement in Circulation is unambiguous: obesity leads to cardiovascular disease and cardiovascular mortality independent of other cardiovascular risk factors. The full list of well-documented independent health consequences, type 2 diabetes, hypertension, fatty liver disease, obstructive sleep apnea, osteoarthritis, several cancers, shortened life expectancy, is extensive, as compiled in a 2025 review in Diabetes, Obesity and Metabolism. Acknowledging these consequences is not a form of stigma. Pretending they do not exist in the name of compassion is not a kindness.
What You Can Do Starting Now
1. Assess your actual metabolic risk today. Measure to waist-to-height ration. If your waist circumference exceeds half your height, make an appointment with your physician and ask specifically for a metabolic evaluation.
2. Begin reducing ultra-processed foods. The goal at the beginning is not perfection, is reduction. For every ultra-processed item in your regular diet, identify one whole-food alternative that you can realistically prepare and enjoy. Start with the meal where ultra-processed food is most dominant and make one replacement there. The evidence base on UPFs is consistent enough that even partial reduction produces measurable benefit.
3. Prioritize sleep as a metabolic intervention. Research consistently links short sleep duration to increased caloric intake, preferential craving for high-reward foods, and impaired metabolic regulation. Assess what is limiting your sleep and address it: screen time before bed, irregular sleep schedules, sleep apnea that has never been evaluated, and chronic stress are the most common culprits. Aim for seven to nine hours of sleep daily.
4. Introduce structured movement. The evidence on physical activity and metabolic health is unambiguous: even modest, consistent movement significantly improves insulin sensitivity, reduces visceral fat, lowers blood pressure, and improves lipid profiles. The American Heart Association recommends at least 150 minutes per week of moderate-intensity aerobic activity, roughly 22 minutes per day, as a minimum threshold for cardiovascular and metabolic benefit. If that feels out of reach at the start, shorter sessions of 10–15 minutes are still metabolically meaningful and a legitimate starting point. The goal is consistency before intensity, walking is sufficient. Walking after meals, in particular, has well documented benefit for post-meal blood sugar control.
Remember to consult your physician before starting any exercise program to determine if it is safe for you.
5. Address stress deliberately. Chronic cortisol elevation drives visceral fat, insulin resistance, and systemic inflammation. Evidence-based stress reduction approaches including mindfulness-based stress reduction (MBSR), regular physical activity, adequate sleep, and social connection, have documented physiological effects on cortisol levels and metabolic markers. If your stress load is driven by circumstances that require structural change (financial, relational, occupational), is important to implement strategies to address them as soon as possible.
6. If psychiatric factors are in the picture, address them directly. If depression, anxiety, or a history of trauma is contributing to the pattern described above, treating those conditions is essential in the treatment of your metabolic health. Food is used as an emotional regulator by many people, often without full awareness, and often as a learned response to environments where other forms of comfort were unavailable. Working with a qualified mental health professional is a necessary intervention.
7. Engage your physician as an active partner. Time constraints in modern medical practice mean that the conversation about metabolic health often does not happen in the depth it deserves. You can change that by showing up with specific questions: Where am I on the metabolic risk spectrum? What are my fasting glucose and HbA1c? Do I have insulin resistance? What screening tests do I need? The physician-patient relationship works best when you are an informed, active participant rather than a passive recipient.
Found this article useful? Share your thoughts. Join the conversation below.
Educational content on The Metabolic Archives is free, because medical information should be accessible to everyone. If you find value and want to support the work, a paid subscription is available and genuinely appreciated. Visit the About Page for additional information.
Disclaimer: The information provided in The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.