
The GLP-1 Miracle
The Science Behind the Drug Reshaping Metabolic Medicine


September 21, 1948 a 29-year-old woman known to history only as Mrs. G, lay bedridden in Saint Marys Hospital in Rochester, Minnesota. Severe rheumatoid arthritis had stripped her of the ability to care for herself independently. That morning, under the direction of physicians Philip Hench and Edward Kendall, she received her first injection of Compound E, a synthetic steroid that would later be called cortisone. Three days later, she was markedly improved. Within a week, she had taken a three-hour shopping trip. Her words to her doctors: “I have never felt better in my life.”
Medicine has witnessed a handful of moments like this when a discovery lands with such force that the profession and the public both struggle to absorb what they are seeing.
Where It Began, The Gut Talks to the Pancreas
The story of GLP-1 begins with a deceptively simple observation. When you eat a meal and glucose enters your bloodstream, your pancreas releases insulin to manage it. Researchers had understood that mechanism for decades. What they had not fully appreciated was that the gut itself actively participates in that signal.
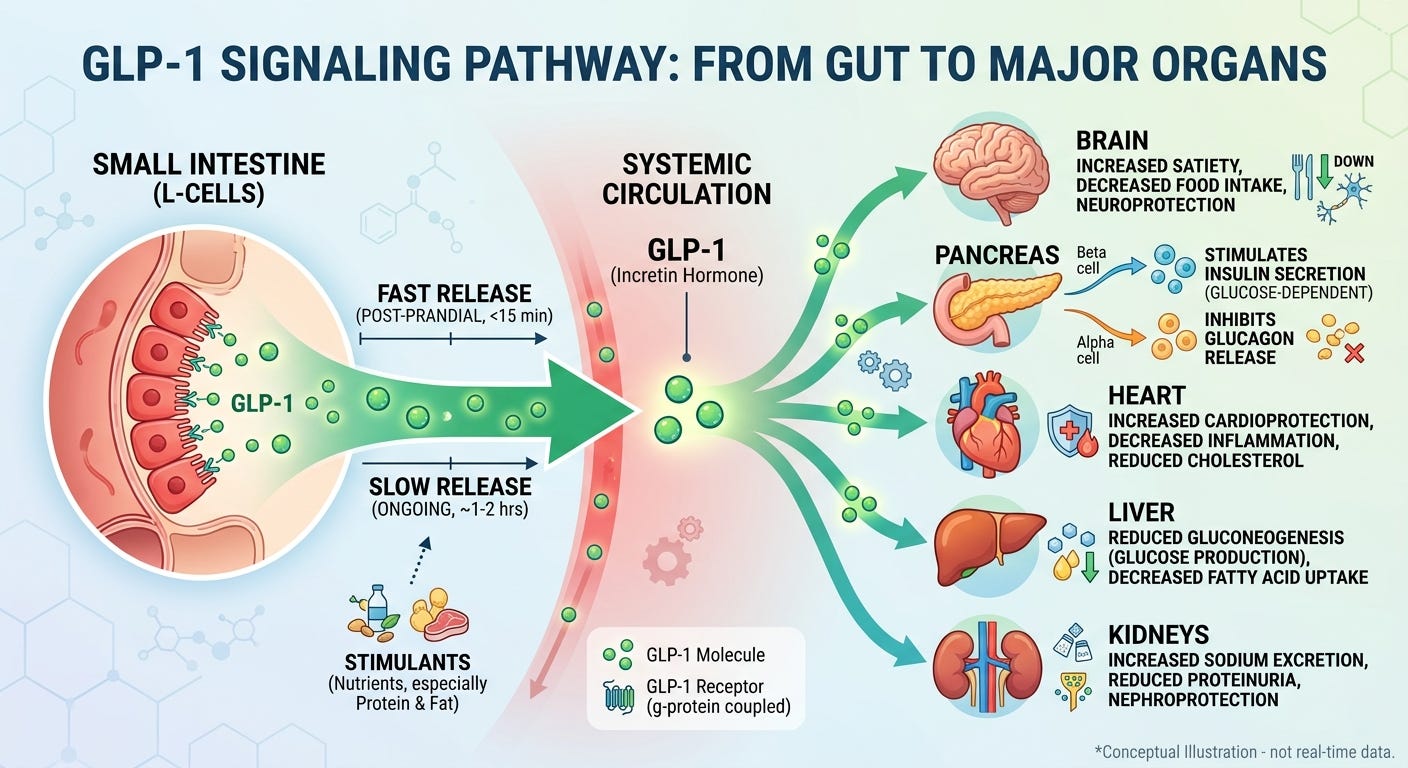
The phenomenon is called the incretin effect: oral glucose produces a substantially greater insulin response than the same amount of glucose delivered directly into the bloodstream. As Baggio and Drucker described in their foundational 2007 review in Gastroenterology, glucagon-like peptide-1 (GLP-1) is the primary messenger responsible for this effect. It is produced by the L-cells of the distal small intestine and colon in response to food intake, and travels through the bloodstream to receptors throughout the body including the pancreas, brain, heart, liver, and kidneys.
The problem is the body degrades its own GLP-1 within approximately two minutes. A hormone that disappears before it can be clinically useful is of limited therapeutic value. The solution arrived from an unlikely source.
The Gila Monster Detour
The Gila monster, a large, venomous lizard native to the American Southwest, produces a compound in its saliva called exendin-4. Structurally, it is remarkably similar to human GLP-1. Functionally, there is a critical difference: the enzyme that destroys GLP-1 in minutes cannot break down exendin-4. Exenatide (Byetta), synthesized from exendin-4, became the first GLP-1 receptor agonist approved by the FDA in 2005, as Sharma and colleagues documented in International Immunopharmacology in 2018. The lineage from lizard saliva to semaglutide, the active molecule in Ozempic and Wegovy, runs in a straight line through two decades of pharmaceutical refinement aimed at a single goal: a compound that mimics GLP-1 durably enough to be therapeutically useful.
How GLP-1 Works, The Pancreas
GLP-1 receptor agonists stimulate insulin secretion from the pancreas only when blood glucose is already elevated. When glucose is normal, the signal quiets. This glucose-dependent mechanism is the reason these drugs do not cause hypoglycemia (low blood glucose) the way older diabetes medications do.
The drugs also suppress glucagon, the hormone released from alpha cells that ordinarily raises blood sugar between meals. In people with type 2 diabetes, glucagon is chronically elevated, contributing to persistently high fasting glucose. GLP-1 receptor activation pulls that glucose release back toward normal.
Finally, they slow gastric emptying, the rate at which food leaves the stomach and enters the small intestine. Nutrients absorbed more gradually produce a shallower, more manageable rise in blood glucose after meals.
If you enjoy evidence-based medical information, subscribe to receive these articles delivered to your mailbox every week.
How GLP-1 Works, The Brain and Food Noise
GLP-1 receptors exist throughout the brain: in the hypothalamus and brainstem, which regulate hunger and satiety, and in the brain’s reward circuitry, including the nucleus accumbens and the ventral tegmental area.
GLP-1 receptor activation in the hypothalamus and brainstem produces satiety signals and does so before a meal is finished, not after. A 2024 study published in Science by Kim and colleagues identified specific neurons in the dorsomedial hypothalamus that encode what researchers call preingestive satiation. GLP-1 receptor agonists amplify these neurons specifically during eating.
GLP-1 receptors in the reward centers modulate dopamine signaling reducing the motivational and emotional pull of food. This is the neuroscience behind what patients describe as food noise going quiet.
Food noise is the intrusive, repetitive mental preoccupation with food that many people with obesity experience as a cognitive and emotional compulsion. A 2025 review in PMC describes this as dysregulation of the brain’s default mode network and reward circuits. For many patients on GLP-1 medications, this signal diminishes or disappears entirely. This food noise is one reason why obesity is so difficult to manage through behavioral intervention alone.
The mechanism for GLP-1’s brain effects is strong in animal models and supported by emerging human neuroimaging data. Circuit-level specificity in humans continues to be established. A 2025 PMC review on GLP-1 modulation of craving and addiction characterizes the state of the evidence accurately: the broad framework is well-supported; some of the more granular claims remain areas of active investigation.
How GLP-1 Works, The Heart and Blood Vessels
GLP-1 receptors are expressed in heart muscle cells and the cells lining blood vessel walls. The drugs suppress inflammatory markers including TNF-α and IL-6, inhibit the formation of arterial plaques, stimulate nitric oxide production in endothelial cells, and reduce oxidative stress.
The clinical confirmation of this is the SELECT trial. Lincoff and colleagues, publishing in the New England Journal of Medicine in 2023, demonstrated that semaglutide 2.4mg weekly produced a 20% reduction in major adverse cardiovascular events over a mean follow-up of 34 months, in patients with obesity and established cardiovascular disease but without type 2 diabetes. Crucially, a pre-specified analysis of SELECT published in The Lancet in 2025 established that only approximately 33% of this cardiovascular benefit was attributable to reductions in waist circumference, at least two-thirds of the protection comes from mechanisms beyond weight loss itself.
Both the American College of Cardiology and the European Society of Cardiology now carry Class I, Level A recommendations for GLP-1 receptor agonists in patients with type 2 diabetes and established cardiovascular disease. These drugs appear to protect the heart and blood vessels through their own direct biological action not merely through weight reductions.
How GLP-1 Works, The Liver
Metabolic dysfunction-associated steatotic liver disease (MASLD), formerly called non-alcoholic fatty liver disease or NAFLD or just fatty liver is the most prevalent chronic liver disease worldwide, affecting an estimated 38% of the global population. It is driven by the same constellation of insulin resistance, excess visceral fat, and systemic metabolic dysfunction that GLP-1 medications address.
In August 2025, the FDA granted accelerated approval to semaglutide 2.4mg weekly for the treatment of MASH (metabolic dysfunction-associated steatohepatitis) the more severe inflammatory stage of the disease with moderate to advanced fibrosis. The approval was based on the phase 3 ESSENCE trial. As reported in updated AASLD Practice Guidance published in Hepatology in 2025, at 72 weeks, 62.9% of patients achieved resolution of steatohepatitis without worsening of fibrosis, compared to 34.3% on placebo. Fibrosis improvement was achieved in 36.8% versus 22.4% on placebo. Both primary endpoints reached high statistical significance.
There is an important nuance worth understanding, the liver does not express significant GLP-1 receptors. The hepatic benefits are mediated indirectly through the drug’s systemic effects on insulin sensitivity, weight, inflammation, and lipid metabolism, operating through the brain, gut, adipose tissue, and pancreas.
How GLP-1 Works, The Kidneys
The organ-protective effects of GLP-1 therapy extend further still. The FLOW trial demonstrated a 24% reduction in major kidney disease events with semaglutide 1mg weekly in patients with type 2 diabetes and chronic kidney disease, as documented in a 2025 PMC review on cardiovascular-kidney-metabolic syndrome management. The renal benefits appear to be mediated through improvements in blood pressure, inflammation, and metabolic dysfunction rather than through direct kidney GLP-1 receptor action, though research in this area continues.
GLP-1 therapy is no longer accurately described as a diabetes drug with a weight loss benefit. It is increasingly understood as a systemic metabolic intervention with organ-protective effects across multiple systems simultaneously.
The Next Generation: Tirzepatide and Dual Agonism
Tirzepatide, sold as Mounjaro for type 2 diabetes and Zepbound for obesity, adds a second mechanism to GLP-1 receptor activation. It also activates receptors for GIP, glucose-dependent insulinotropic polypeptide, another incretin hormone with overlapping but non-identical distribution in the brain and peripheral tissues. The synergy between these two receptor pathways appears to produce greater weight loss than GLP-1 activation alone.
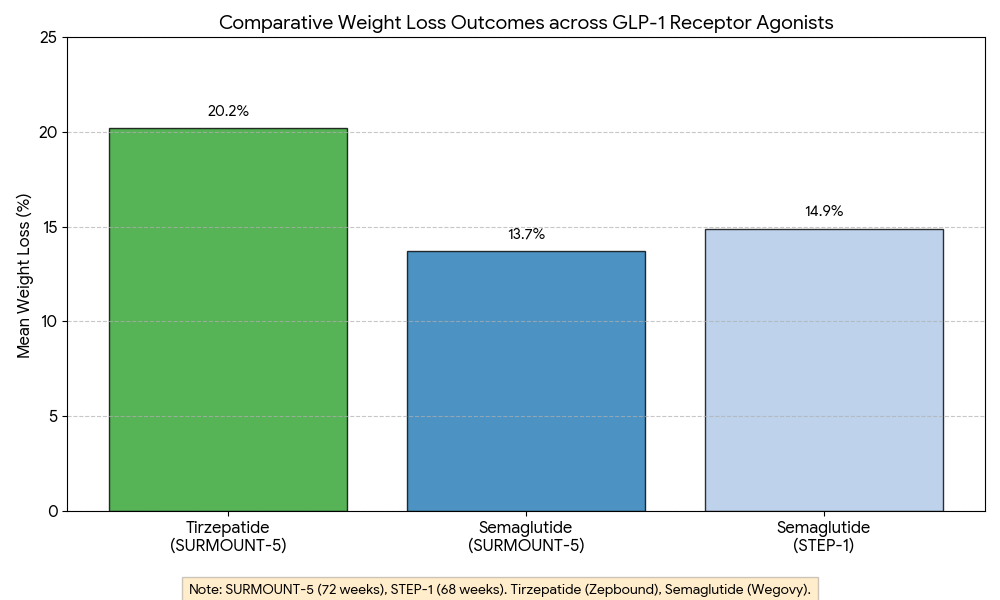
The SURMOUNT-5 trial, published in the New England Journal of Medicine in May 2025, was the first direct head-to-head comparison of tirzepatide against semaglutide in patients with obesity without type 2 diabetes. Aronne and colleagues reported that tirzepatide produced 20.2% mean body weight loss versus 13.7% for semaglutide at 72 weeks, a 47% greater relative reduction. Nearly twice as many tirzepatide participants achieved 25% or greater weight loss. The gastrointestinal side effect profiles were broadly comparable, though tirzepatide showed slightly higher rates of treatment discontinuation due to GI effects (5.6% versus 2.7%). Is worth pointing out this trial was open-label and funded by Eli Lilly, maker of Tirzepatide.
The precise mechanism by which adding GIP agonism amplifies weight loss remains under active investigation. If this trial results are to be taken at face value (paint me a skeptic here), it suggests dual receptor activation produces outcomes approaching those previously seen only with bariatric surgery.
Side Effects and the Discontinuation Reality
The most common adverse effects are gastrointestinal: nausea, vomiting, diarrhea, constipation. These are dose-dependent, most prominent during the dose escalation phase, and resolve or diminish for most patients over time. Rare but serious side effects include acute pancreatitis, symptomatic gallbladder disease, acute kidney injury from dehydration in the context of severe GI symptoms, and progression of diabetic retinopathy in patients with pre-existing retinopathy. A 2024 review by Tobaiqy in Endocrinology and Metabolism Clinics of North America provides a systematic account of the serious adverse event profile from trial and real-world data.
Studies in rodent receiving high doses of GLP-1 exhibited thyroid C-cell hyperplasia and increased rates of medullary thyroid carcinoma (MTC). That potential concern led to an FDA black box warning on semaglutide products. Is important to note that thyroid C-cells in rodents express GLP-1 receptors at higher density than in humans. While no evidence of increased incidence of MTC associated to GLP-1 drugs has been noted in humans so far, the scientific community remains vigilant.
The STEP-4 trial established that stopping semaglutide leads to reversal of most metabolic benefits, including substantial weight regain, within months (Wilding et al., NEJM, 2022). A 2025 systematic review and nonlinear meta-regression by Budini and colleagues on medRxiv confirmed the trajectory of regain following cessation of GLP-1 receptor agonists. A 2026 analysis by Shah and colleagues in Diabetes, Obesity and Metabolism addressed the clinical management implications.
The underlying metabolic dysfunction that the drug manages does not disappear when the drug stops. For most patients with significant metabolic disease, GLP-1 therapy is a lifelong commitment, not a defined course of treatment with an end point.
These are powerful tools and need to be used with the same care and precision that the science behind them reflects. Part 2 examines what that means in practice and what happens when it doesn’t.
Found this article useful? Share your thoughts. Join the conversation below.
Educational content on The Metabolic Archives is free, because medical information should be accessible to everyone. If you find value and want to support the work, a paid subscription is available and genuinely appreciated. Visit the About Page for additional information.
Disclaimer: The information provided in The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.