
The Silent Epidemic: Understanding Type 2 Diabetes
Part One: How a silent metabolic disruption develops into diabetes.


Look around the next waiting room you sit in, pharmacy line, cardiac unit, dialysis center, or surgical recovery ward. Diabetes is present in all of them so prevalent it no longer registers as alarming.
According to the CDC’s National Diabetes Statistics Report (updated January 2026) about 12% of Americans have diabetes today, and two in five have pre-diabetes. The majority do not even know it.
For most people with type 2 diabetes the disease has been quietly building for years and could have been interrupted long before any diagnosis was made.
What Is Diabetes
At its most fundamental level, diabetes is an imbalance between insulin activity and insulin requirements.
Insulin is the hormone your pancreas produces to manage blood glucose. When your body’s cells stop responding to insulin efficiently (a state called insulin resistance), the pancreas compensates by releasing more insulin to keep glucose levels normal.
Eventually the pancreas can no longer keep up and blood glucose begins to rise. At a certain point those numbers cross thresholds we label as pre-diabetes, then type 2 diabetes. Those thresholds are diagnostic criteria derived from population-level statistical data not biological events. The damage begins well before the number crosses these lines.
The window for the most effective intervention is open years before most patients, or even clinicians, act on it.
Common Diabetes Types
Type 1 Diabetes is an autoimmune disease that destroys the insulin-producing cells of the pancreas. It is not the focus of this series.
Gestational Diabetes on the other hand, is not a pregnancy complication that resolves at delivery, it is the unmasking of pre-existing metabolic vulnerability. While pregnancy normally cause some insulin resistance, in at-risk women it exposes significant pre-existing insulin resistance leading to abnormal glucose levels. Most GDM patients already have some degree of obesity and known family history of type 2 diabetes. Women with gestational diabetes carry approximately a 50% risk of developing type 2 diabetes within 5–10 years if the underlying metabolic dysfunction is not addressed.
This makes the postpartum window a critical and time-sensitive intervention opportunity.
Type 2 Diabetes Mellitus is the quintessential metabolic disease, and is what the rest of this article will focus on.
The Scale of the Problem

According to the CDC’s January 2026 data, 40.1 million Americans have diabetes diagnosed and undiagnosed combined, representing approximately 12% of the US population. Of those roughly 11 million are estimated to be undiagnosed. Another 115.2 million American adults are estimated to have prediabetes, with 80% of them unaware of their status.
Estimates among Americans aged 60 and older, more than 27% have diabetes and more than 52% have prediabetes, per NCHS Data Brief No. 516, published November 2024. That is more than half of the over-60 population at elevated metabolic risk.
The ADA’s definitive economic analysis, published in Diabetes Care in November 2023, calculated the total annual cost of diabetes in the United States at $412.9 billion; $306.6 billion in direct medical costs and $106.3 billion in indirect costs including reduced productivity, disability, and premature death. People with diabetes account for one in four healthcare dollars spent in this country. The average annual medical expenditure per person with diabetes is $19,736, 2.6 times higher than for a comparable person without diabetes.
The GBD 2021 Diabetes Collaborators, publishing in The Lancet in June 2023, project that global diabetes prevalence will more than double by 2050, affecting over 1.3 billion people. In the United States modeling by CDC researchers projects that diabetes prevalence could reach 25–33% of the adult population by 2050 under middle-ground scenarios.
If you enjoy evidence-based medical information, subscribe to receive these articles delivered to your mailbox every week.
How the Healthy Body Manages Blood Sugar
Note: This is a simplified account of mechanisms that in reality involve dozens of interacting molecular pathways, multiple organ systems, and decades of ongoing research. The goal here is clarity.
When you eat carbohydrates are broken down into glucose and absorbed into the bloodstream. Your pancreas detects the glucose rise and releases insulin in two distinct waves, what physiologists call a biphasic response.
The first wave is a rapid burst of pre-formed insulin released within minutes of glucose entering the bloodstream. Its job is to suppress the liver’s own glucose production and prime peripheral tissues to start receiving glucose. The second wave is a sustained continuing insulin secretion that manages the ongoing glucose load from the meal.
We now know the gut is hormonally active and plays an active role in blood glucose regulation. Hormones called incretins, released when food enters the small intestine, amplify the pancreatic insulin response. Research has established that the incretin effect accounts for approximately 50% of insulin release after oral glucose ingestion.
Insulin opens the doors to glucose uptake across three key tissues. In the liver, insulin signals cells to store glucose and suppresses the liver’s own glucose production. In muscle, the body’s largest glucose consumer, insulin triggers the movement of specialized transport proteins called GLUT4 to the cell surface allowing glucose to enter. In fat tissue insulin promotes glucose and fat storage and suppresses the breakdown of stored fat. Insulin is also the body’s primary anabolic hormone, besides glucose storage, it drives fat synthesis and increases lean body mass.
Opposing insulin is glucagon, produced by a different set of cells in the pancreas. Glucagon raises blood glucose when it falls too low triggering the liver to release stored glucose. The balance between insulin and glucagon is what keeps blood glucose within a narrow normal range.
Muscle cells can take up glucose through a completely separate pathway that doesn’t require insulin, activated by physical contraction. This insulin-independent GLUT4 activation in exercising muscle is one of the most important reasons for exercise as a fundamental therapeutic strategy.
How the Disease Develops
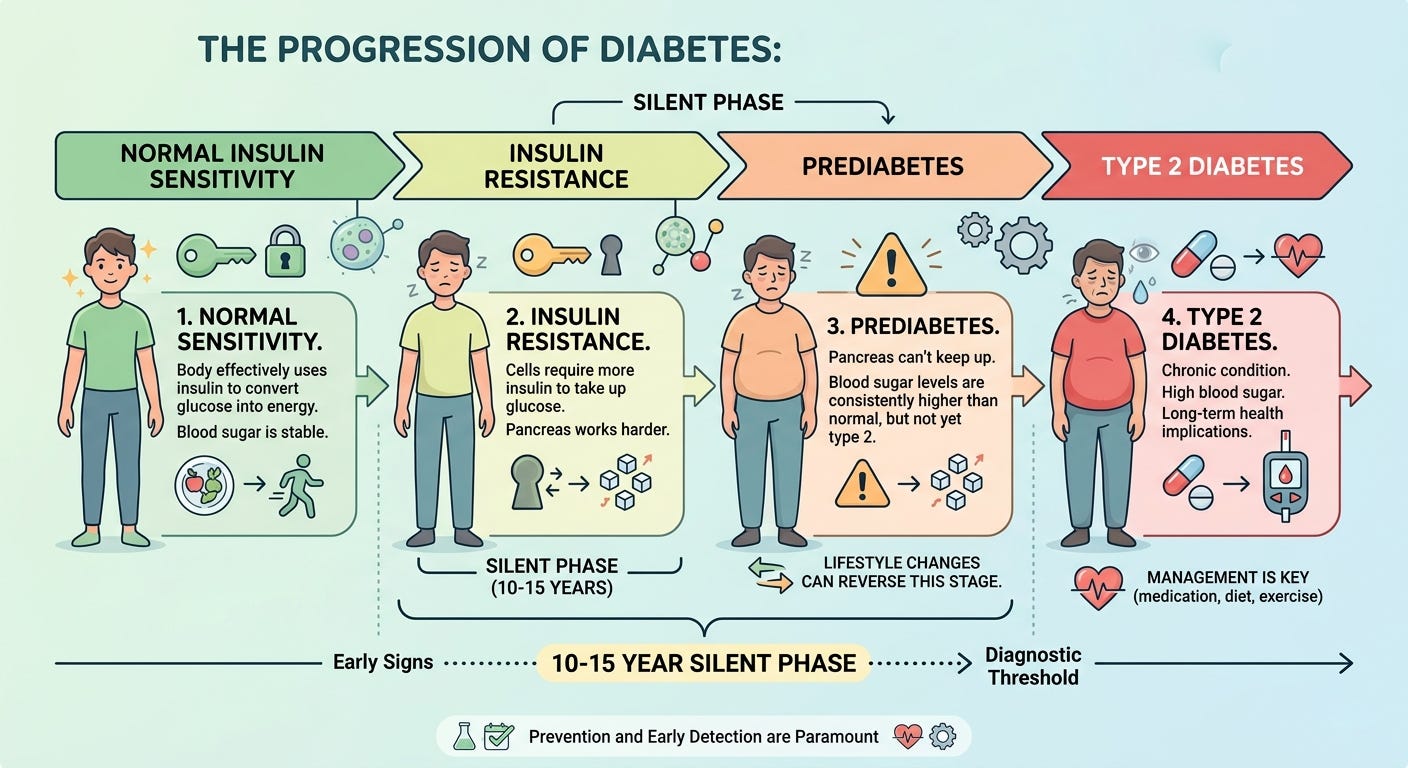
Act One: The Silent Phase
Insulin resistance is thought to precede the diagnosis of type 2 diabetes by 10 to 15 years according to StatPearls’ 2023 clinical review. The pancreas produces higher amounts of insulin to overcome the increasing tissue resistance keeping blood glucose in a normal range.
Act Two: The Initiating Insult
One of the primary driver of insulin resistance is visceral fat, deposited around the abdominal organs.
Subcutaneous fat, the kind you can pinch, has no significant metabolic risk. As peripheral fat stores become full, fat depositing internally around the organs. Visceral fat is metabolically active and pro-inflammatory.
Research has established visceral adipose tissue as the leading factor in type 2 diabetes risk, independent of overall BMI. Visceral fat drains directly into the portal vein, which feeds the liver. The liver becomes exposed to increased concentrations of free fatty acids and inflammatory molecules leading to increased hepatic insulin resistance.
Act Three: Three Tissues Breaking Down
As insulin resistance deepens, the three key target tissues fail in sequence. The liver stops responding to insulin’s signal and begins releasing glucose even when it isn’t needed. Muscle cells take up less glucose after meals. Fat tissue begins releasing fatty acids into the bloodstream rather than storing them.
All these events lead to rising levels of circulating blood glucose, particularly after meals. In spite increasing circulating insulin levels, blood glucose starts to climb: this is the pre-diabetic stage.
Act Four: Beta Cell Exhaustion
The pancreas has been compensating through all of this by producing more and more insulin to overcome the resistance. But the beta cells that produce insulin are not inexhaustible. The landmark work of Dr. Ralph DeFronzo, published in Diabetes in 2009, established that subjects with years of pre-diabetes may have already lost more than 80% of functional beta cell capacity by the time diabetes is diagnosed.
The loss of first-phase insulin secretion is one of the earliest detectable defects. This removes the brake that normally suppresses the liver’s glucose production before a meal has even been digested, leading to progressive rise in post meal glucose levels and eventually elevations of the fasting glucose levels as well.
Act Five: The Cycle Reinforces Itself
As insulin resistance becomes established a new dynamic takes hold: insulin resistance and obesity became mutually reinforcing processes. Obesity drives insulin resistance; eventually insulin resistance drives obesity. Chronically elevated insulin is a potent fat-storage signal that actively resists fat mobilization. Emerging evidence suggests that hyperinsulinemia itself may drive further insulin resistance becoming a self-reinforcing cycle where the disease progressively makes itself harder to treat.
The increasing difficulty losing weight once insulin resistance is fully established is partially driven by these reinforcing processes.
What This Means for You
Eight things worth holding onto from this discussion:
Type 2 diabetes is not a sudden event, is the endpoint of a process that began silently years earlier.
Visceral fat is the primary initiating insult for most patients. Body weight is an incomplete indicator of metabolic risk; where fat is deposited matters as much as how much.
The diagnostic thresholds, while useful for classification and staging, are not a defining boundary of biological events. Meaningful intervention should begin when the metabolic risk profile warrants it not when a number crosses a line on a lab report.
Gestational diabetes is not just a pregnancy complication that resolves at delivery. It is the unmasking of pre-existing metabolic vulnerability in at-risk women, leading to Type 2 Diabetes years later if not addressed.
Metabolic disruption does not stay contained it propagates across organ systems. Understanding this interconnection is the foundation of understanding why early intervention is not optional.
Pre-diabetes is reversible with targeted intervention. Early type 2 diabetes is remission-capable in appropriate candidates when meaningful beta cell reserve remains. Advanced type 2 diabetes with significant beta cell exhaustion narrows that window considerably. Earlier intervention, when peripheral fat develops, is always better.
Lifestyle modification is the fundamental treatment to reverse insulin resistance. The landmark Diabetes Prevention Program trial demonstrated a 58% reduction in progression from pre-diabetes to type 2 diabetes through intensive lifestyle intervention, compared to 31% with metformin making it more effective than the best available medication for this purpose.
Diet and exercise recommendations form your doctor are not a dismissal of your condition, are the most effective medical intervention known for pre/diabetes and metabolic diseases in general.
The mechanisms described in this article do not remain confined to blood glucose numbers. They reach the eyes, the kidneys, the nerves, the heart, and the feet. The damage is not random, and it is not bad luck. The next articles in this series examines what that damage looks like, why it occurs, and why the timeline for prevention is almost always longer than patients realize.
Found this article useful? Share your thoughts. Join the conversation below.
Educational content on The Metabolic Archives is free, because medical information should be accessible to everyone. If you find value in it and want to support the work, a paid subscription is available and genuinely appreciated. Visit the About Page for additional information.
Disclaimer: The information provided in The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.