
What’s Wrong with Medicine Today: My Perspective After Forty Years in the System
How Reimbursement Policy Reshaped the Practice of Medicine | Part Four

OPINION PIECE
The harsh reality about how American healthcare works: how physicians and hospitals are paid determines how they behave. This is an observation that applies across every industry, institution, and professional class; medicine is not exempt from it.
The history of Medicare reimbursement policy since 1965 is one of the clearest available demonstrations of this principle. It is a forty-year sequence of payment reforms, each designed to correct the behavioral distortions of the previous model, each producing its own new set of distortions in turn.

Cost-Plus Reimbursement and the Incentive to Spend
Medicare back in 1965 reimbursed hospitals on a cost-plus basis: the hospital submitted its costs, Medicare paid those costs plus a margin. Every dollar spent returned a dollar plus profit. Prolonging services and expanding billing increased reimbursement. There was no financial penalty for inefficiency and no financial reward for restraint.
Many hospitals and physicians responded to this incentive as economic theory predicts: services were prolonged, billing was expanded. According to the Commonwealth Fund’s 2015 analysis of Medicare payment reform, annual Medicare spending per beneficiary rose from $472 in 1975 to $1,579 in 1985 a growth rate of 12.8% per year, or 5.3% adjusted for inflation.
The third-party payers and eventually Medicare raised legitimate concerns. The reform response was predictable.
The DRG and the Incentive to Discharge
The Social Security Amendments of 1983 established the Medicare Prospective Payment System based on Diagnosis-Related Groups (DRGs). Hospitals would receive a fixed payment per admission determined by the patient’s primary diagnosis, regardless of the actual costs incurred. Efficient hospitals retained the surplus, while hospitals whose costs exceeded the DRG payment absorbed the loss.
Average inpatient length of stay fell sharply following implementation, and Medicare Part A spending per beneficiary declined in the post-1983 period (Commonwealth Fund, 2015). The DRG had accomplished what it was designed for: it redirected the financial incentive from prolonging stays to shortening them.
The incentive to discharge efficiently and the incentive to discharge at the clinically appropriate moment are not the same. The prospective payment system was explicitly designed to give hospital administrators tools to influence individual physician discharge decisions (Fetter and Thompson, Yale University; cited in OIG HHS, OEI-09-00-00200).
Utilization Review Committees. These were hospital-based committees, required as a condition of Medicare participation, whose mandate was to review admissions and lengths of stay against established criteria. The committee reviewed physician decisions about admission and discharge against financial benchmarks and had authority to flag cases for further review or challenge clinical necessity determinations.
Physician-specific practice pattern data. The hospital’s internal data systems, fed by Medicare billing records, could generate reports showing each physician’s average length of stay by DRG compared to the hospital average and the national benchmark. That data was visible to administration and became the basis for what were called utilization management conversations, that in practice ranged from informal pressure to formal credentialing consequences in some institutions.
If you enjoy evidence-based medical information, subscribe to receive these articles delivered to your mailbox every week.
RVUs, the AMA, and the Systematic Devaluation of Primary Care Medicine
The Resource-Based Relative Value Scale (RBRVS), authorized by Congress through the Omnibus Budget Reconciliation Act of 1989 and implemented in 1992, was designed to establish physician payment across specialties. The previous standard produced wide and largely arbitrary payment variability. The RBRVS replace it with a structured system in which each physician service was assigned a relative value unit (RVU) reflecting the time, skill, and resources required, and reimbursement would follow from that value.
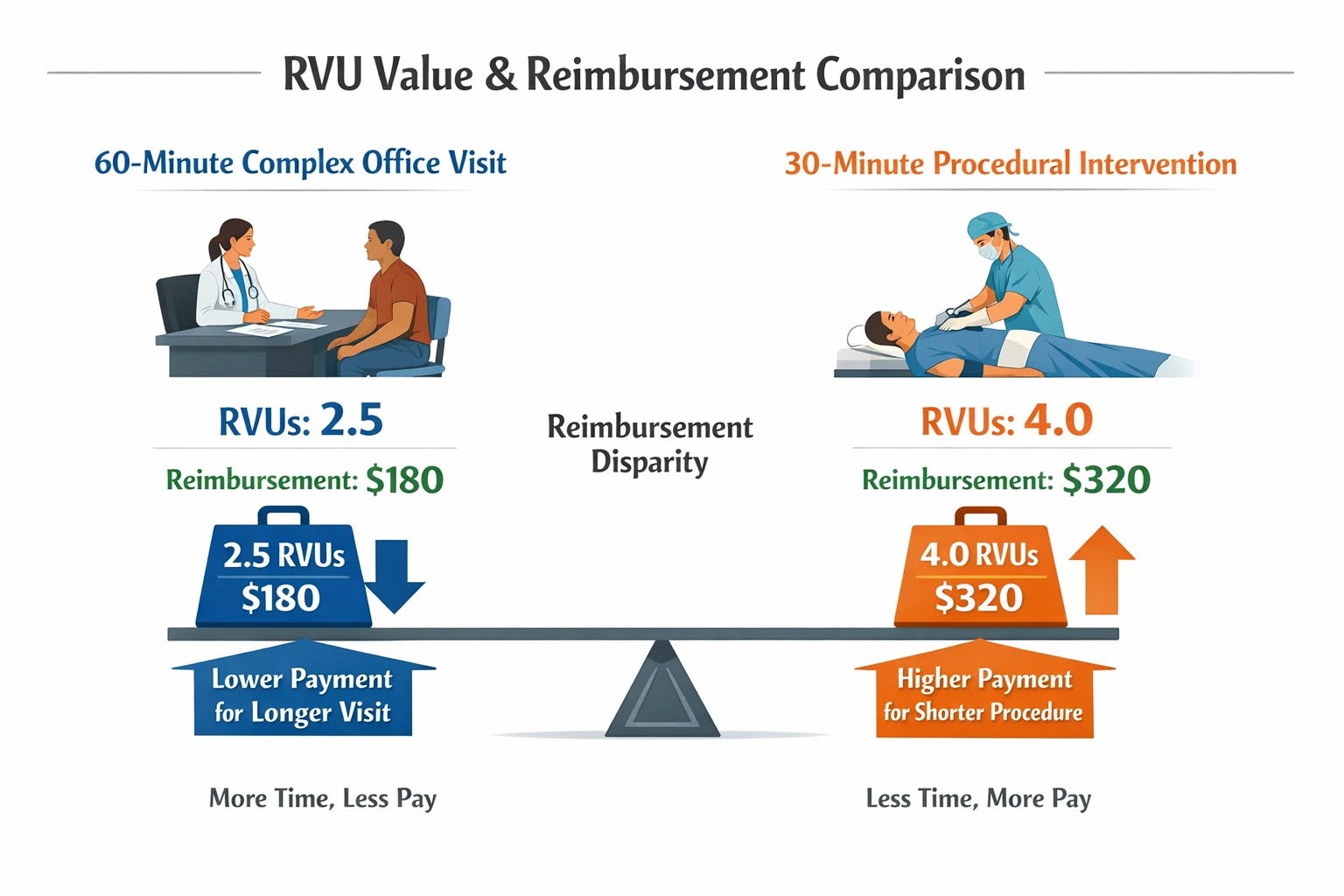
Procedural intervention was systematically overvalued relative to primary care service. The reimbursement system does not reward what the most vulnerable patients need from their physician the most — time spent. It is a documented, persistent, and repeatedly criticized feature of the RVU schedule that the Medicare Payment Advisory Commission (MedPAC) and multiple independent analyses have identified and that the system has declined to correct (Laugesen, Fixing Medical Prices, Harvard University Press, 2016; PMC11977100).
The American Medical Association holds intellectual property rights to the Current Procedural Terminology (CPT) coding system. Every claim submitted to Medicare, Medicaid, and private insurance uses a CPT code. That code ownership generates royalty revenue for the AMA on the order of tens of millions of dollars annually (Laugesen, 2016).
The AMA’s Specialty Society Relative Value Scale Update Committee is a private physician committee, heavily weighted toward procedural specialists, whose recommendations to the Centers for Medicare and Medicaid Services (CMS) on RVU values are accepted in the large majority of cases. The RUC effectively determines how much each physician service is worth within the Medicare payment system, without the regulatory transparency requirements that apply to other government bodies.
The organization that owns the coding system controls the committee that determines the relative financial value of each code. This represents a conflict of interestthat has been allowed to persist for more than three decades.
The Assembly-Line Consequence: What RVU Undervaluation Looks Like in the Waiting Room
Primary care is the most cognitively intensive, least procedural domain in medicine. It is also, within the RVU framework, among the most financially disadvantaged relative to its overhead costs and clinical complexity demands.
The independent primary care physician facing overhead costs that consistently outpace per-encounter reimbursement has one available response within this system: increase encounter volume. More patients per day means less time per patient. Less time per patient means abbreviated encounters that cannot adequately address the increasingly complex medical care is expected to manage.
The system then compounds this by defining quality partly through metrics — preventive care completion rates, chronic disease control targets, medication adherence scores — that require exactly the time the reimbursement model makes financially unsustainable to provide. The physician is caught between what the metrics demand and what the economics permit.
The Mandate Response and the Hospital Readmissions Reduction Program
The Hospital Readmissions Reduction Program (HRRP), enacted as part of the Affordable Care Act in 2010 with financial penalties beginning in fiscal year 2013, is the most consequential case study in this pattern.
The stated goal was to reduce preventable hospital readmission; the financial driver: 3.3 million readmissions annually at an associated cost of $41.3 billion made reducing readmission a fiscal priority for CMS as much as a clinical one (Navathe et al., PMC6105419, 2018).
The HRRP created financial penalties for hospitals whose 30-day readmission rates for specified conditions exceeded risk-adjusted national benchmarks. By fiscal year 2017, 79% of acute care hospitals in the United States were subject to HRRP penalties, with up to 3% of a hospital’s entire inpatient Medicare reimbursement at risk (Navathe et al., PMC6105419). The program generated $528 million for CMS in fiscal year 2017 alone.
There is no financial reward within the HRRP for improvement. As national readmission rates decline over time, the benchmark moves with them, meaning hospitals face penalties even when they demonstrably reduce their own rates.
The Conflicting Mandate Trap: When Two Rational Policies Become One Irrational System
The DRG prospective payment system created a financial incentive to shorten hospital stays. The HRRP created a financial penalty for patients who return within 30 days of discharge. For the straightforward patient, an efficient discharge with adequate follow-up avoids unnecessary returns. For the typical Medicare beneficiary, with multiple interrelated chronic conditions, these conflicting goals are oftentimes irreconcilable.
The Unintended Consequences: What the Evidence Actually Shows
The penalty structure fell disproportionately on safety-net hospitals serving dual-eligible Medicare-Medicaid patients. Poverty and associated social health determinants independently increase readmission risk regardless of the quality of care provided. The HRRP risk-adjustment models did not adequately account for these factors, meaning these hospitals were effectively penalized for serving the patients most likely to be readmitted irrespective of care quality (Joynt and Jha, PMC4231573, 2014).
The mortality data is more troubling still. Four independent studies identified an association between HRRP implementation and increased 30-day mortality among heart failure patients, the program’s primary target population (Dharmarajan et al., PMC6589834, 2019; Gupta et al., JAMA Internal Medicine, 2021). The finding prompted Congress to mandate a formal review under the 21st Century Cures Act. The studies identified a temporal correlation between the program’s implementation and a mortality increase, did not prove the program caused the increase.
Penalty savings accrued to CMS while safety-net hospitals were financially weakened. This contradictory mandate system may have saved money in aggregate while concentrating the harm on the hospitals that serve the most vulnerable populations. Whether that constitutes a defensible policy outcome is a judgment I leave to the reader.
The Step-Down Facility Gap

Medicare patients discharged to skilled nursing facilities face a 25% likelihood of readmission or death within 30 days. In a review of 200 SNF discharges, 67% of readmissions were rated as potentially preventable, with patients reporting that inadequate facility care contributed to the majority of returns (Mack et al., PMC6069909, 2018). Across more than 1.5 million Medicare SNF discharges, facilities with the lowest staffing ratings had combined 30-day readmission or death rates of 25.5%, compared to 19.8% at the highest-staffed facilities (Kramer et al., PMC4203396, 2014).
The full examination of what skilled nursing facilities are, what they are not, and what patients and families need to understand before entering one belongs to the next piece in this series. What
The Honest Accounting
The cost pressures that drove each successive reform are real, documented, and threatening to the long-term fiscal sustainability of Medicare. The medical profession contributed to those pressures through the exploitation of cost-plus reimbursement that made reform both necessary and politically achievable. The architects of the DRG system, the RBRVS, and the HRRP were not indifferent to patient welfare, most were trying to improve it.
The policies examined here were designed for a population, but the unintended consequences are experienced by the individual.
Found this article useful? Share your thoughts. Join the conversation below.
Educational content on The Metabolic Archives is free, because medical information should be accessible to everyone. If you find value and want to support the work, a paid subscription is available and genuinely appreciated. Visit the About Page for additional information.
The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.
The systemic inefficiencies you point out fail everyone in the American healthcare and it's sad. From what you've mentioned here, patients aren't positive they'll get the best care they need, and the physicians who care about their patients aren't able to provide the best support that they can.