
What’s Wrong with Medicine Today: My Perspective After Forty Years in the System
Turning the Finger on Ourselves | Part Eight

OPINION PIECE
This piece is an account of decades spent inside the profession witnessing our collective failures. This indictment is self-inclusive, treated with the same intellectually honest standard I have strived for elsewhere.

Nothing that follows changes a fundamental truth: the majority of physicians entered medicine to serve patients and continue doing so despite increasing constraint, diminishing authority, and mounting personal cost. It provides accountability the profession at large.
The Original Sin
Cost-plus reimbursement, the dominant payment model through much of the postwar period, rewarded volume, duration, and expenditure without reference to outcome. A portion of the profession responded with excess: extended hospital stays, procedures without clear indications, frequency of follow-up appointments for stable conditions. The payment reforms that followed were institutional responses to physician-driven cost inflation.
Cesarean Section Explosion
The cesarean section rate climbed from approximately 5% in 1970 to over 32% today. The mechanism is documented in peer-reviewed literature: when fertility declined through the 1970s and early 1980s, reducing obstetricians’ volume of vaginal deliveries, cesarean rates increased in direct proportion. A nationally representative dataset shows a strong within-state correlation between fertility decline and cesarean rate increase during this period, consistent with an induced demand model (Gruber and Owings, RAND Journal of Economics, 1996). Women delivering at hospitals generating higher profit per cesarean procedure were significantly more likely to undergo cesarean delivery than women at lower-profit hospitals (JAMA Network Open, 2021, PMC7980096).
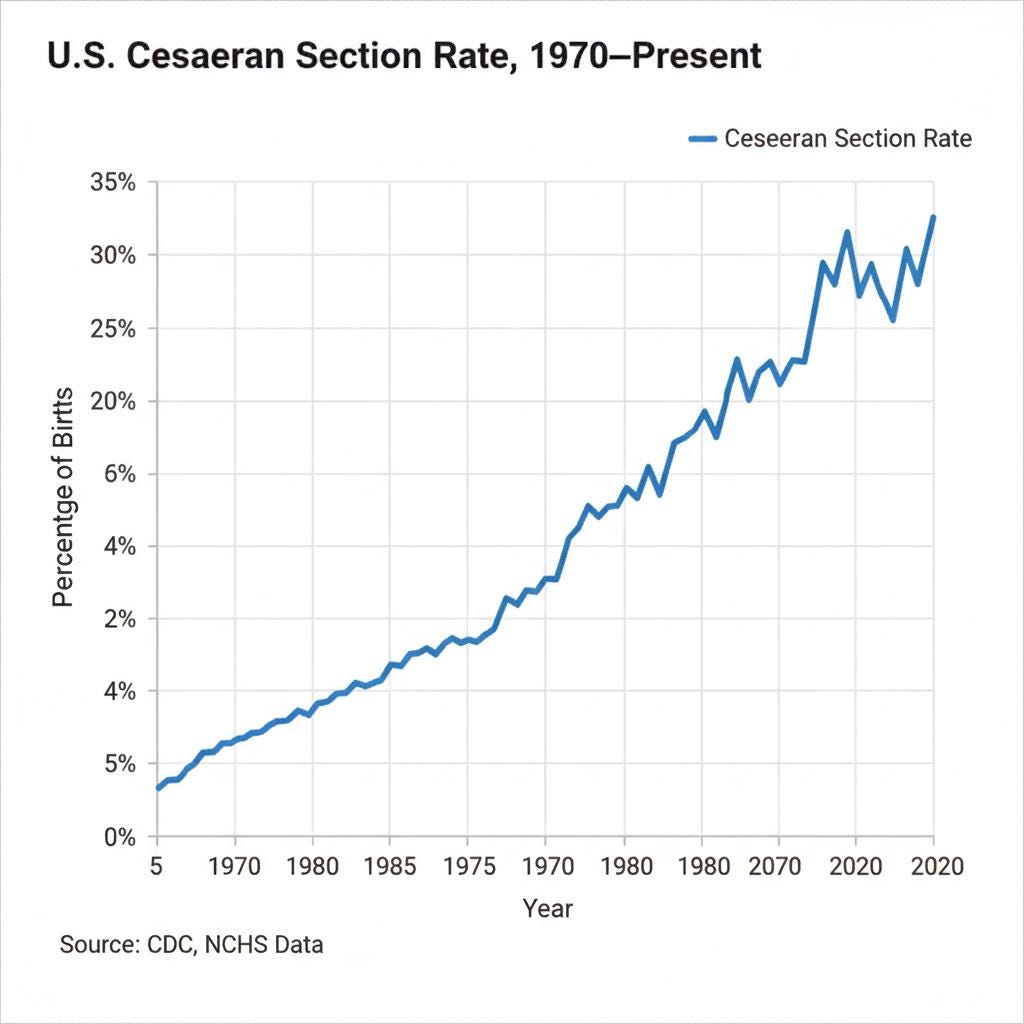
The American College of Obstetricians and Gynecologists has itself stated that the rapid increase in cesarean rates without concomitant improvement in maternal or neonatal outcomes raises significant concern about cesarean delivery overuse.
Multiple drivers beyond profit operate simultaneously: liability fear, patient preference, scheduling convenience.
If you enjoy evidence-based medical information, subscribe to receive these articles delivered to your mailbox every week.
The Reactive Response
When reimbursement model changed, the profession adapted. The RVU architecture undervalued primary care rewarding procedures instead. The response in many practices was to compress encounter time and increase daily patient throughput. This “assembly-line” practice was a choice made by physicians responding to financial pressures.
The consequence for patients was abbreviated encounters with reduced depth of clinical engagement, and the erosion of the therapeutic relationship.
The Ownership Conflict
Other practices adopted a different model in response to the financial pressures.
Physician ownership of ancillary services creates a direct and financial conflict of interest. The physician who owns in-house laboratory equipment, imaging technology, stress testing facilities, DEXA scan units, or ECG and X-ray equipment has a financial incentive to order more of these services. Physician-owned facilities order significantly more ancillary services than non-physician-owned ones for identical patient populations (Medicare Payment Advisory Commission, MedPAC, 2005; Iglehart, New England Journal of Medicine, 2005).

The federal government recognized this conflict of interest as consequential enough to require legislative response. The Stark Law was the result: it prohibits physician self-referrals for Medicare and Medicaid designated health services.
As a result other arrangements were developed for continued capture of economic benefits from self-referral while technically complying with the law. Some of those include: management services organizations, indirect compensation arrangements, and space and equipment rental structures. Those represent legally creative efforts pushing the limits of the law.
Defensive Medicine Costs
The threat of liability for failing to order a test, to refer, or to pursue an intervention a patient demanded, contribute to measurable costs increases through over utilization.
The most conservative peer-reviewed estimate puts defensive medicine costs at approximately $46 billion annually, representing roughly 2.9% of total healthcare spending at the time of measurement (Mello et al., Health Affairs, 2010). Nine out of ten physicians in a national survey reported practicing defensive medicine (Jackson Healthcare, 2010). In a Massachusetts study of internists, 27% of CT scans, 16% of laboratory tests, and 14% of hospital admissions were reported as ordered due to concerns about liability rather than clinical indication (BMJ Quality and Safety, 2014, PMC4231873).
Defensive medicine takes two forms:
Assurance behavior: ordering additional services to document clinical thoroughness and reduce liability exposure. I admit being guilty of this practice.
Avoidance behavior: declining high-risk procedures or clinical situations where liability exposure is elevated, producing access problems in obstetrics, neurosurgery, and emergency medicine.
Fragmentation as Professional Culture
The expansion of subspecialty referral has contributed to patient care fragmentation. The drivers are multiple: liability fear, the RVU undervaluation of primary care work, time pressure, and, in some cases, the financial architecture of referral relationships within physician networks.
The result: complex patient accumulates multiple specialists, medication lists grow, testing is duplicated across specialties with no coordinating clinician tracking the entire picture.
The Continued Medical Education Industry
Approximately 28,000 to 46,000 active peer-reviewed medical journals now exist worldwide. Collectively they publish between 1.8 and 3 million articles annually. PubMed adds approximately 800,000 to 1 million new citations per year. A physician attempting to maintain current knowledge across even a single specialty would need to read dozens of relevant articles daily, across hundreds of distinct journals.
Many busy physicians, myself included, depend on formal CME programs and digest publications to maintain professional competency. Many of these are partially or totally funded by device manufacturers, pharmaceutical companies or healthcare systems. They usually concentrate on education promoting drugs over non-financially viable treatments, and limit discussion of emerging non-commercial alternatives. They drive physician behavior and become the basis for the accepted standards of care that effectively govern the practice of medicine.
CME industry sponsorship accounts for approximately 50–65% of total CME revenue in the United States, representing more than $1 billion annually from pharmaceutical and device manufacturers (Lexchin, Canadian Family Physician, 2006, PMC2231419; Lexchin and Sekeres, Canadian Family Physician, 2014, PMC4131951). The industry estimates it recoups $3.56 in increased sales for every dollar invested in CME.
Sponsored CME increases prescribing rates for the sponsoring company’s products. In one analysis, positive clinical effects of the sponsoring drug were mentioned 2.5 to 3 times more often than competitor drugs during sponsored educational sessions (Bowman and Pearle, Journal of Continuing Education in the Health Professions, 1988). Physicians who interact more frequently with industry sponsored CME have poorer prescribing habits and lower rates of evidence-based guideline adherence (Avorn and Shostack, Circulation, 2010).
The Case of Oxycontin
Between 1996 and 2002, Purdue Pharma sponsored more than 20,000 educational programs disseminating information that misrepresented OxyContin’s addiction risk. These programs were funded by the pharmaceutical company, led by industry-sponsored physicians, and accredited by professional bodies. OxyContin sales grew from $48 million in 1996 to $1.1 billion in 2000.
The educational programs were a covert promotional strategy, the epidemic that followed was the public health consequence.
Accountability Without Absolution
The majority of physicians choose medicine to serve patients despite existing systemic limitations. Nothing in this piece is meant to diminish the genuine dedication and sacrifices most of them bring to patient care.
Is meant as an intellectually honest acknowledgment of the profession’s failures, as well as my own. A well overdue reckoning of our collective participation in the healthcare system’s failures.
Found this article useful? Share your thoughts. Join the conversation below.
Educational content on The Metabolic Archives is free, because medical information should be accessible to everyone. If you find value and want to support the work, a paid subscription is available and genuinely appreciated. Visit the About Page for additional information.
The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.