
What’s Wrong with Medicine Today: My Perspective After Forty Years in the System
When money talks, we all loose | Part Ten

OPINION PIECE
Money drives behavior is the proposition running through this series. Today we explore the reverse: when money drives the changes. Will take a look of how money shapes healthcare policy.
Lobbying Is Not the Problem
Lobbying is a constitutionally protected right.
“Congress shall make no law respecting an establishment of religion, or prohibiting the free exercise thereof; or abridging the freedom of speech, or of the press; or the right of the people peaceably to assemble, and to petition the Government for a redress of grievances.”
— First Amendment, Bill of Rights, US Constitution
In principle is the mechanism by which the people can voice their positions to elected representatives. The problem is when money is the one making the petition instead.
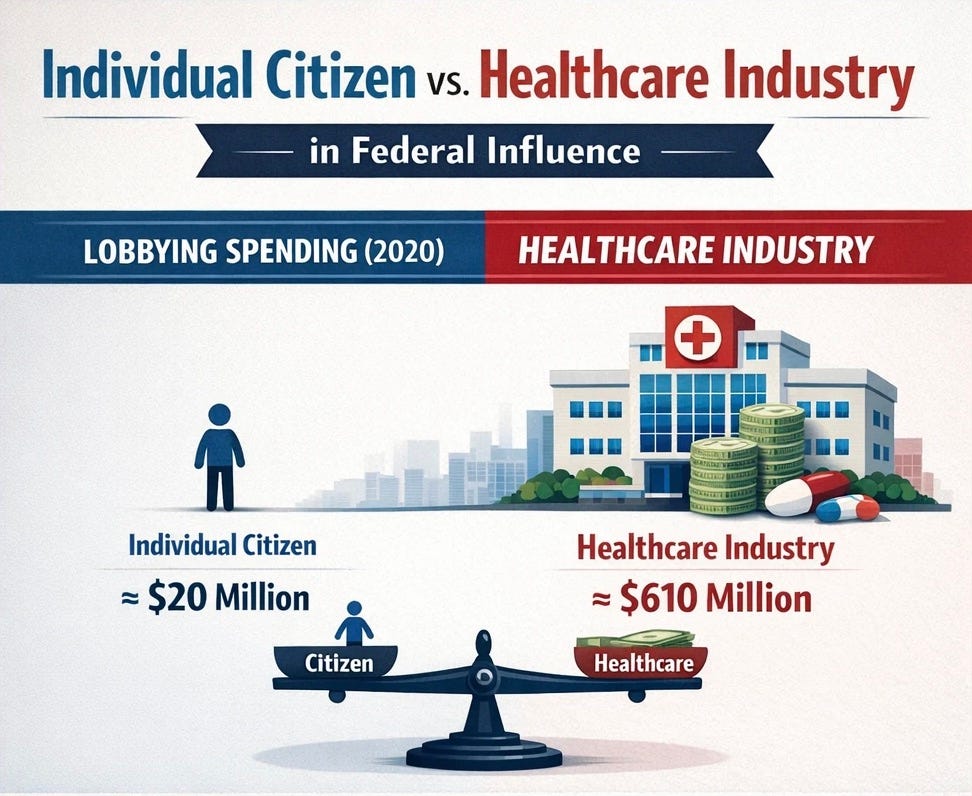
Total healthcare sector lobbying expenditures grew from $358 million in 2000 to $714 million in 2020, a 70% increase over two decades (Wouters OJ et al., JAMA Health Forum, 2022). In 2021, the sector spent nearly $700 million, the highest ever recorded in a single year. The breakdown by subsector in 2020: pharmaceutical and health product manufacturers led at $308 million, providers at $287 million, and payers at $81 million. Spending is highly concentrated, the top 10% of firms account for 70% of payer lobbying expenditures and 69% of manufacturer expenditures. The healthcare sector has ranked among the top five lobbying spenders in the United States consistently for decades. In 2009 alone, more than $1.1 billion was spent lobbying the initial version of what would become the Affordable Care Act (Center for Public Integrity, 2010).
The Industry is Party Agnostic
The overall health sector has shifted its giving between parties multiple times over the past three decades, favoring Republicans in some cycles, Democrats in others, always consistently following power rather than ideology (OpenSecrets, Health Sector Summary).
The insurance industry has historically favored Republicans. The pharmaceutical industry historically favored Republicans as well, then flipped toward Democrats in 2020, and has distributed nearly evenly since. In the 2023-2024 election cycle, pharmaceutical PACs gave $5.2 million to Democrats and $6.6 million to Republicans (PharmaVoice, October 2024). Individual major companies split their contributions deliberately across both parties’ congressional and senatorial committees. Novo Nordisk gave 49% to Democrats and 51% to Republicans. Eli Lilly divided its giving evenly between both parties’ committees (BioSpace, August 2024).
Seven of the top ten organizations registered to lobby on the Inflation Reduction Act were pharmaceutical or health insurance companies (OpenSecrets, 2022).
Both parties have been recipients of healthcare industry money across every administration and every Congress for fifty years, and both parties have consistently failed to enact structural reform of the system that funds them.

Who Represents Patients?
According to peer-reviewed analysis of federal tax disclosures and organizational reporting, 67.3% of patient advocacy organizations receive industry funding (Rose SL et al., JAMA Internal Medicine, 2017). Nearly 12% receive more than half their total funding from industry. More than one third have pharmaceutical, biotech, or medical device executives on their boards of directors. Only 12% have published conflict of interest policies. A separate analysis published in the New England Journal of Medicine found that of 104 large patient advocacy organizations examined, one stated plainly that it accepted no industry funding (McCoy MS et al., NEJM, 2017). One.
Between 2010 and 2022, the pharmaceutical industry distributed at least $6 billion in grants to more than 20,000 organizations, more than it spent on direct lobbying and campaign contributions combined during the same period (KFF Health News, December 2023). Funding concentrates in disease categories where the contributing company has commercial products, not in areas where patients most need advocacy.
The answer to the original question “who represents patients in the policy process?” is sadly, nobody.
If you enjoy evidence-based medical information, subscribe to receive these articles delivered to your mailbox every week.
The ACA: What Happened, What It Produced
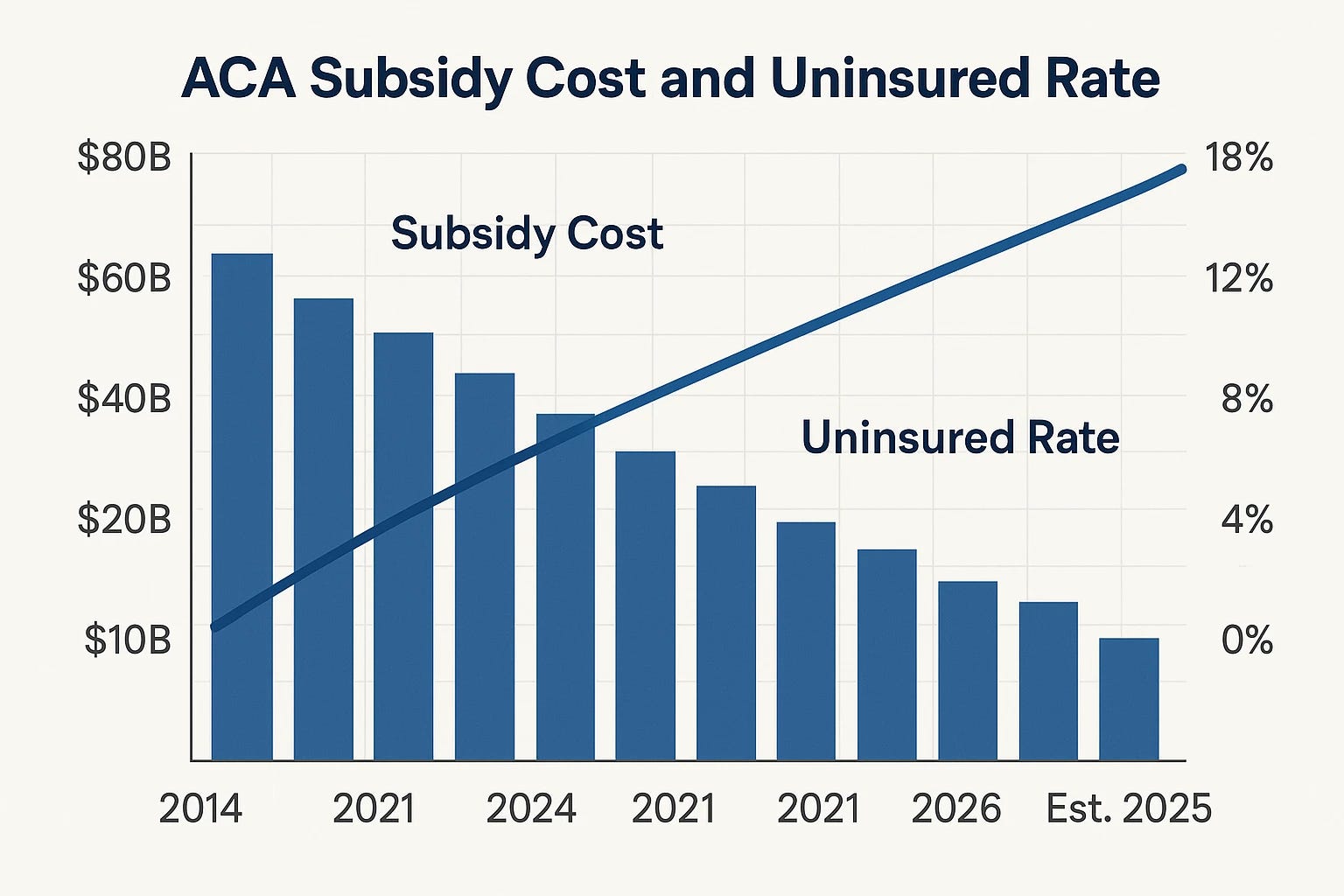
The Affordable Care Act produced real coverage gains. The uninsured rate fell from 14.5% in 2013 to a record low of 7.7% in 2023. The number of uninsured Americans dropped from 45.2 million to 26.4 million. Twenty million previously uninsured Americans gained coverage (KFF, October 2025; CBPP, March 2024).
What is also true is the cost trajectory. The gross federal cost of ACA marketplace subsidies grew from $18 billion in 2014 to $92 billion in 2023 and an estimated $138 billion in 2025 (Committee for a Responsible Federal Budget, November 2025). The Congressional Budget Office projects total federal subsidies for health insurance will reach $25 trillion over the 2024-2033 decade (CBO, September 2023). Out-of-pocket costs for insured Americans rose 77% over the decade despite expanded coverage. The individual mandate was effectively eliminated in 2019 when the tax penalty was reduced to zero, altering the legislation’s economic architecture without repealing the legislation itself.
As of 2022, 26.4 million Americans remained uninsured. Thirty percent of providers deny Medicaid patients, limiting access to the coverage that was expanded. The structural incentives driving healthcare cost growth were not altered by the ACA’s passage.
But Who Shaped It?
When the Senate Finance Committee took the lead in drafting the ACA the legislation was primarily written by Elizabeth Fowler, Senator Max Baucus’s chief health policy counsel. Before joining his office, Fowler had served as Vice President for Public Policy and External Affairs at WellPoint, at the time the nation’s largest health insurance provider. After the ACA passed, she moved to the White House to oversee its implementation. She subsequently left for a senior-level position in Johnson & Johnson’s government affairs and policy group (The Guardian, December 2012).
The pharmaceutical industry, through PhRMA, supported the ACA publicly while lobbying specifically to exclude Medicare drug price negotiation authority. The insurance industry, through AHIP, publicly supported the ACA while internally spending approximately $100 million to limit its most disruptive provisions. (ProPublica; OpenSecrets, June 2021). The version of the ACA that passed preserved the employer-sponsored insurance system, prohibited Medicare from negotiating drug prices, and did not include a public option. Each of these outcomes aligned precisely with the financial interests of the industries that lobbied most heavily during the drafting process.
The COVID Era
Beginning in March 2020, the federal government and state governments implemented economy-wide business closures of a scale and duration without precedent in American peacetime history. Schools closed, affecting tens of millions of children, with documented multi-year consequences for academic achievement and developmental outcomes. Mask mandates were implemented at federal, state, and local levels with varying legal authority, enforcement mechanisms, and durations. Vaccine mandates were implemented for specific employment categories, one of the best examples was the military mandate.
On August 24, 2021, the Secretary of Defense issued a memorandum requiring all members of the US Armed Forces to receive COVID-19 vaccination. Approximately 17,000 service members refused. More than 8,400 were involuntarily discharged: 3,717 Marines, 2,041 Navy sailors, 1,841 Army soldiers, and 834 Air Force and Space Force members.
Legal challenges were filed on First Amendment, Religious Freedom Restoration Act, and informed consent grounds. Congress directed rescission through Section 525 of the 2023 National Defense Authorization Act. The mandate was rescinded on January 10, 2023. On January 27, 2025, President Trump signed an executive order directing reinstatement of those discharged, as of mid-2025, fewer than 200 of the 8,400 discharged had returned to service (Executive Order, January 27, 2025; EANGUS; New Civil Liberties Alliance; Military Times, February 2026).
During the same period, federal health agencies were involved in directing social media content moderation of COVID-related information. The House Select Subcommittee on the Coronavirus Pandemic documented communications between federal health officials and social media platforms regarding the moderation of COVID-related content. Federal courts addressed related First Amendment questions through the Missouri v. Biden litigation. The specific communications are part of the public congressional record (House Select Subcommittee on the Coronavirus Pandemic, Final Report, 2024). The scope, intent, and justification of that involvement remain actively contested in legal and political proceedings.
The COVID era is the most extreme illustration of what happens when government assumes authority over individual healthcare decisions at scale. Any honest evaluation of proposals to expand governmental control over individual healthcare decisions should account for that record.
The Architecture That Sustains the Failures
Across this series we examined what is wrong with the American healthcare system through the behavior of its major players. The political architecture documented in this piece, while not the only cause of all those failures, is the mechanism by which they are sustained.
The concluding piece in this series will bring all these pieces together and offer several coherent proposals to address some of the structural problems identified throughout this series.
Found this article useful? Share your thoughts. Join the conversation below.
Educational content on The Metabolic Archives is free, because medical information should be accessible to everyone. If you find value and want to support the work, a paid subscription is available and genuinely appreciated. Visit the About Page for additional information.
The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.
My health care is great.