
What’s Wrong with Medicine Today: My Perspective After Forty Years in the System
Now You See Me, Now You Don’t | Part Six

OPINION PIECE
Who decide which medications your insurance covers? Who decide what you pay at the pharmacy counter? Who decide which pharmacy you can use without paying a penalty? Not your physician, insurer or drug manufacturer.
It is an entity called a Pharmacy Benefit Manager. The invisible middle man of America’s healthcare system.
The Invisible Hand
Three companies control approximately 80% of prescription benefit management (PBM) in the United States: CVS Caremark, Cigna’s Express Scripts, and UnitedHealth Group’s OptumRx. Together they administer drug benefits for roughly 270 million Americans in a market worth nearly $600 billion annually (Federal Trade Commission, September 2024). These are among the largest corporations in the country.
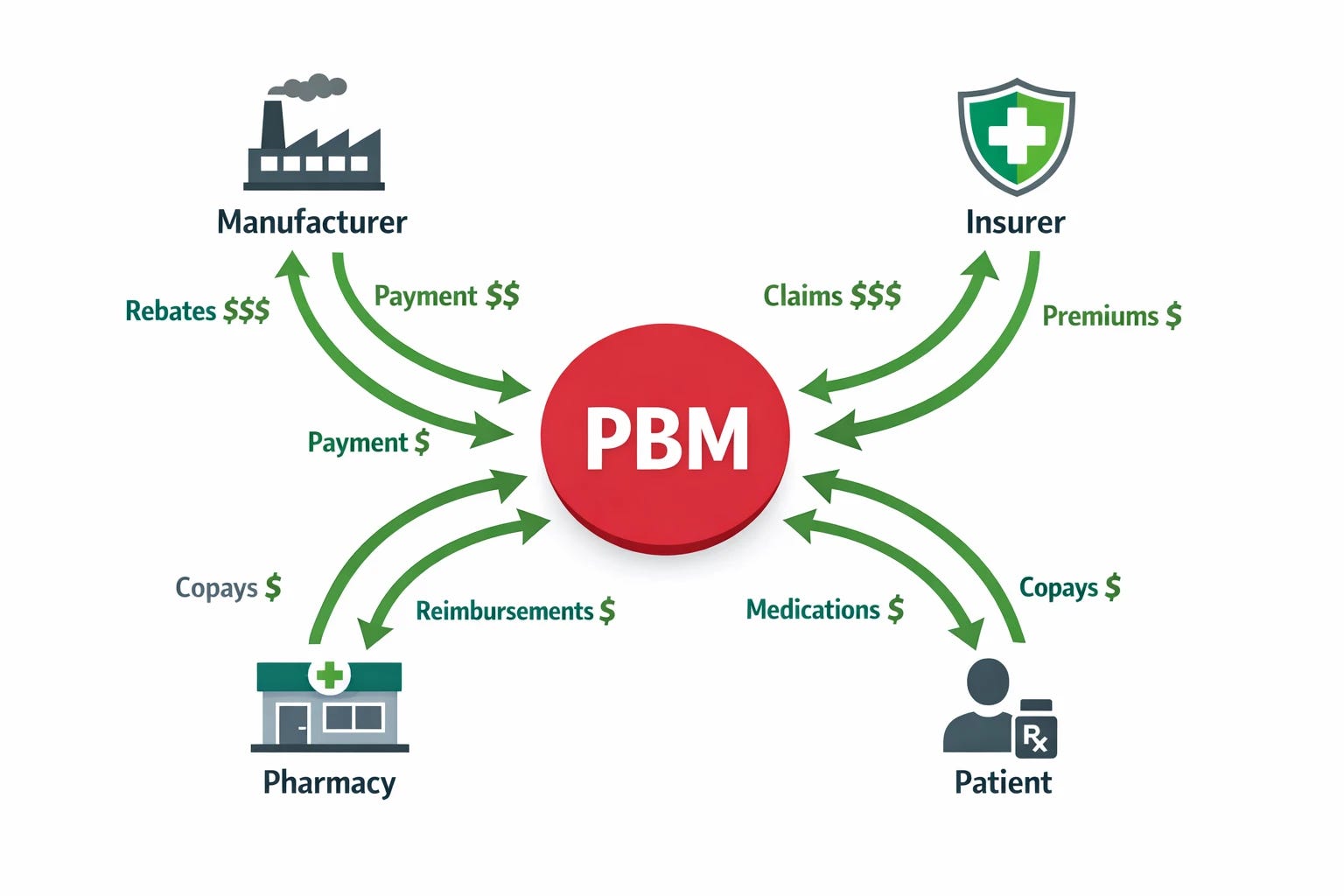
Your employer or insurer contracts with a PBM to manage the prescription drug benefit on their behalf. The PBM then contracts with drug manufacturers to negotiate rebates, contracts with pharmacies to set reimbursement terms, and administers the benefit for every covered member. It sits at the center of every transaction without being visible in any of them.
What PBMs Actually Do
Claims processing at scale: Approximately 4 billion prescription drug transactions occur annually in the United States (Commonwealth Fund, March 2025). Each requires real-time eligibility verification, formulary checking, drug utilization review, prior authorization adjudication, copay calculation, and payment processing across thousands of health plans, tens of thousands of pharmacies, and hundreds of drug manufacturers simultaneously.
Pharmacy network contracting: Negotiating reimbursement terms with tens of thousands of pharmacies nationally is beyond the capacity of any individual health plan. The aggregated purchasing power of a PBM representing 270 million covered lives produces negotiating leverage. In principle, this should reduce costs.
Drug utilization review: Real-time checking of prescriptions for drug-drug interactions, duplicate therapy, dosing errors, and therapeutic alternatives at the point of dispensing catches errors that would otherwise reach patients.

Formulary development: Health plans lack the clinical infrastructure to independently evaluate thousands of drugs across hundreds of therapeutic categories. PBMs employ pharmacy and therapeutics (P&T) committees to perform this evaluation and determine which drugs are covered, at what tier, and under what conditions.
If you enjoy evidence-based medical information, subscribe to receive these articles delivered to your mailbox every week.
Evidence shows that members with pharmaceutical companies relations seating in P&T committees are more likely to request formulary additions of those companies’ drugs (Friesen et al., Journal of Clinical Pharmacy and Therapeutics, 2020). Today CMS requires at least one independent practicing physician and one independent practicing pharmacist free of financial conflicts on these committees (AMCP Partnership Forum, Journal of Managed Care and Specialty Pharmacy, 2023). Only two members without ties to the industry on a committee usually including twenty or more.
How PBMs Make Money
Rebate Retention and the List Price Inflation Cycle
Drug manufacturers pay PBMs rebates in exchange for preferred formulary placement. The rebate is calculated as a percentage of the drug’s list price. The higher the drug’s list price, the larger the rebate the PBM receives. The PBM therefore has a financial incentive to favor drugs with higher list prices over therapeutically equivalent alternatives with lower list prices and smaller rebates.
Manufacturers inflate list prices specifically to fund the rebates PBMs demand for formulary placement. The patient’s copay, deductible, and coinsurance is calculated against the full list price, not the net price after rebate, inflating the patient’s out pocket expenses accordingly. The PBM excludes lower-cost alternatives from the formulary, because a lower list price generates a smaller rebate reducing PBM revenue.
Spread Pricing
For generic drugs, PBMs are reimbursed by health plans and employers at one price and pay pharmacies at a lower price: this difference is retained as profit. The spread is pure margin extracted from the drug transaction with no corresponding service delivered (FTC Interim Report, July 2024; Commonwealth Fund, March 2025).
Vertical Integration
The three largest PBMs are owned by or affiliated with a major health insurer and simultaneously owns its own pharmacy chain. CVS owns Caremark the PBM, Aetna the insurer, and CVS the pharmacy chain. UnitedHealth owns OptumRx the PBM and operates extensive healthcare provider networks. Cigna owns Express Scripts the PBM (FTC, September 2024).
The PBM steers prescriptions to its own pharmacy, charges its own insurer the spread and structures formularies to maximize rebate magnitude. A 2025 study found clear evidence: the share of prescriptions filled at PBM-owned pharmacies was substantially higher among patients enrolled in PBM-owned health plans than among patients covered by other insurers (CSG South, December 2025).
Vertical integration also produces another casualty: the independent community pharmacy. PBMs reimburse their own affiliated chain pharmacies at higher rates than independent pharmacies for identical drugs. Some PBMs exclude independent pharmacies from plan networks entirely. The independent pharmacist is being driven out of business by a reimbursement structure the PBM controls.
The Insulin Case
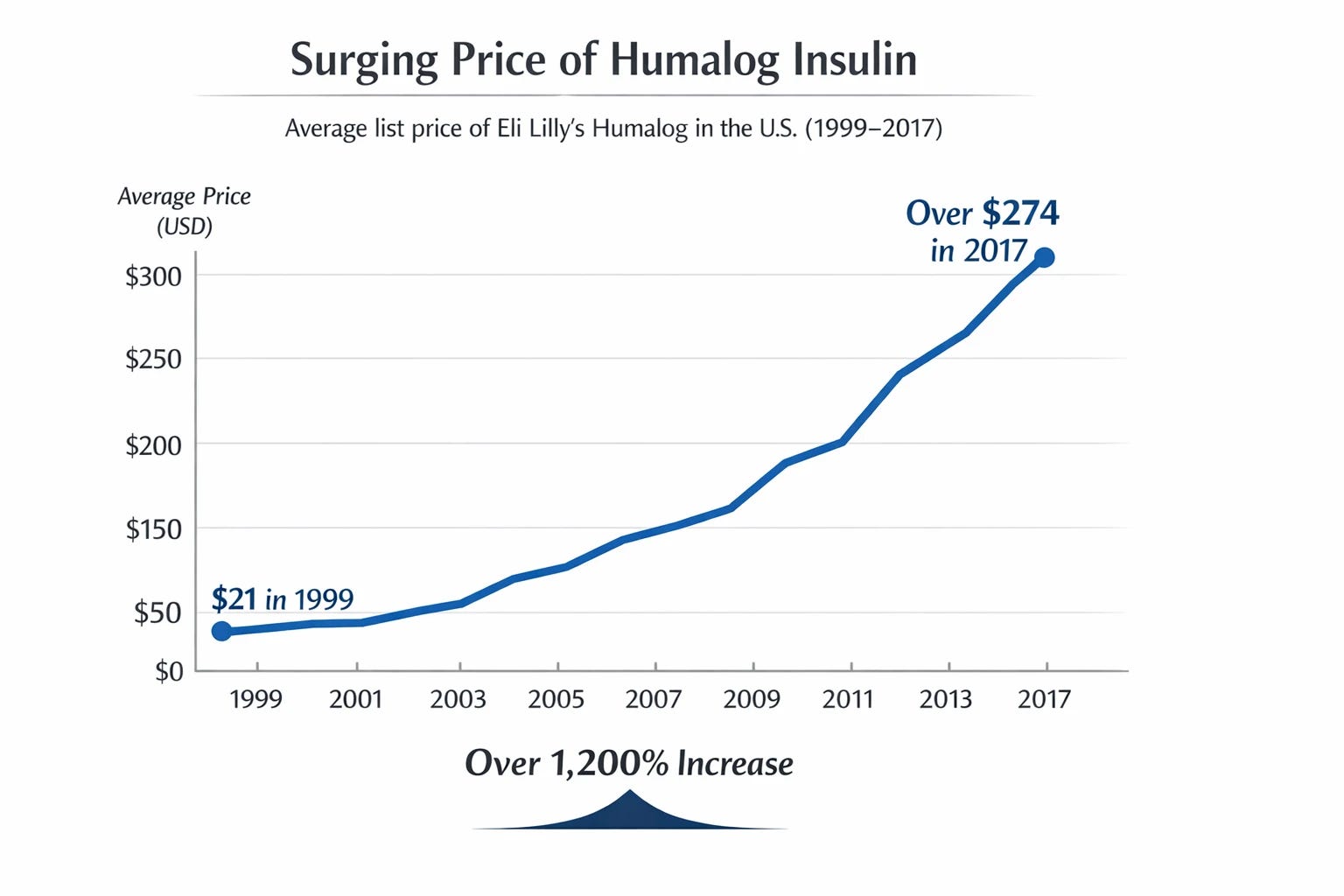
In 1999, the average list price of Eli Lilly’s Humalog insulin was $21. By 2017, it had risen to more than $274, over 1,200% increase (Feldman and Rome, JAMA Network Open, 2023). The production cost for Humalog did not significantly increase during the same period.
The Federal Trade Commission’s administrative complaint, filed September 2024, documents the mechanism. The three largest PBMs pushed insulin manufacturers to compete for preferred formulary coverage based on the size of rebates rather than net price. Manufacturers raised list prices to fund those rebates while PBMs collected billions in rebates and fees. When lower-cost insulin alternatives became available, PBMs systematically excluded them from formularies.
From 2012 to 2019, gross sales for four leading insulin products more than doubled, from $13 billion to $27 billion. Net sales after rebates dropped approximately 40%, from $8 billion to $5 billion. By 2019, the rebates paid exceeded 80% of list price (FTC Administrative Complaint, September 2024). By 2019, one in four insulin-dependent patients in the United States was unable to afford their medication (Fang and Selvin, JAMA, 2023).
In February 2026, the FTC secured a landmark settlement with Express Scripts: it requires separating PBM compensation from list prices, patient out-of-pocket expenses calculated from net prices without rebates, and increased transparency projected to reduce patient out-of-pocket costs for drugs like insulin by up to $7 billion over ten years (FTC, February 13, 2026).
Litigation against CVS Caremark and OptumRx continues. The PBMs have simultaneously filed suit against the FTC challenging its administrative proceedings on constitutional grounds.
What Is Currently Being Done
The FTC’s two-year investigation produced an interim report in July 2024, an administrative complaint against all three major PBMs in September 2024, and the February 2026 Express Scripts settlement. PBM reform is one of the rare legislative territories where Democrats and Republicans have found common cause without giving in to lobbying pressure. State attorney general actions have proceeded in Vermont, California, Kentucky, Ohio, and Hawaii. Federal legislation passed in 2025 requires PBM compensation delinking from drug list prices and mandatory rebate pass-through for Medicare Part D beginning January 1, 2028 (KFF, February 2026; AJMC, March 2026).
The legislation addresses Medicare Part D specifically. The commercial employer market covering approximately 159 million Americans has weaker protections under current law (KFF, February 2026).
What This Means for You
The PBM system was created to solve administrative coordination of prescription drug benefits at national scale but evolved into a mechanism for extracting value from the drug transaction at the patient’s expense. Always in the dark.
You cannot demand accountability from a system you cannot see.
Now you finally can!
Found this article useful? Share your thoughts. Join the conversation below.
Educational content on The Metabolic Archives is free, because medical information should be accessible to everyone. If you find value and want to support the work, a paid subscription is available and genuinely appreciated. Visit the About Page for additional information.
The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.