
What’s Wrong with Medicine Today: My Perspective After Forty Years in the System
Light at the End of the Tunnel | Part Eleven

OPINION PIECE
The question this series has build toward is whether or not the American healthcare system is worth saving. The honest answer is: it depends. Let’s first compare the strengths and weaknesses of our system with the rest of the civilized world. Then present some proposals to correct some of the problems we have analyzed over the course of this series.

Where Our System Fails
The United States ranks last among ten high-income nations on four of five health outcome measures, according to the Commonwealth Fund’s Mirror, Mirror 2024 report, the most comprehensive international health system comparison available, drawing on OECD data, WHO data, and standardized survey methodology across peer nations.
Life expectancy in the US stands at 78.4 years, compared to a ten-country peer average of 82.5 years, a gap of 4.1 years that has widened over the past two decades (Commonwealth Fund, Mirror Mirror 2024, September 2024).
Maternal mortality sits at 18.6 deaths per 100,000 live births, more than three and a half times the peer average of 5.1. This gap holds across every racial, ethnic, socioeconomic, and age group in the country (KFF, International Comparison of Health Systems, October 2025).
Infant mortality is the highest among peer nations.
Preventable and treatable death rates are the highest among peer nations.
The US spends $14,885 per capita on healthcare, more than double the peer average of $7,371, and nearly 50% more than second-place Switzerland at $9,963 (Peterson-KFF Health System Tracker, October 2025). US healthcare expenditure represents 17.6% of GDP against a peer average of approximately 10%. The primary driver is price (PGPF, How Does the US Healthcare System Compare to Other Countries, October 2025).
Where Our System Leads
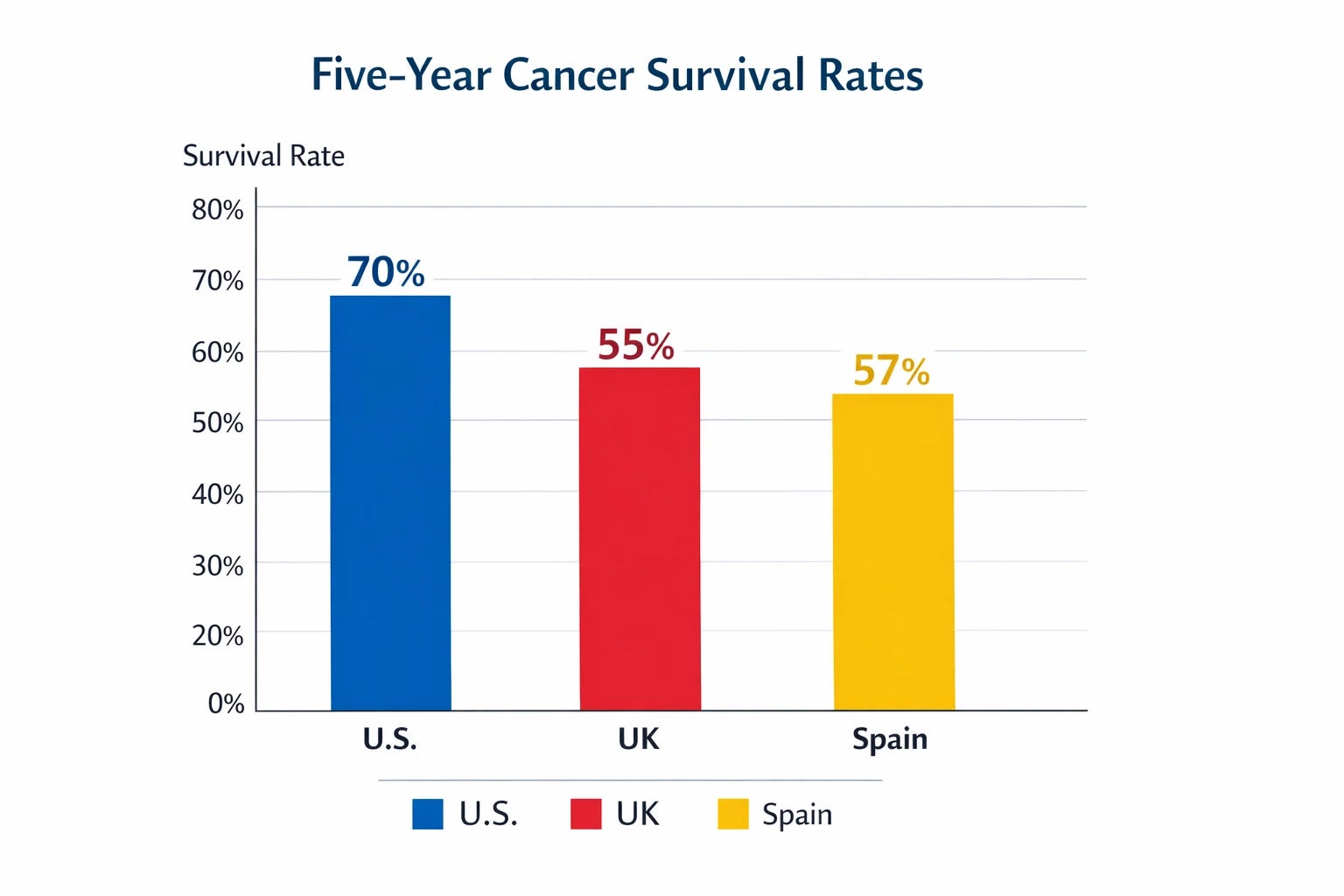
The US all-cancer five-year survival rate is approximately 70%, compared to 55% in the UK and 57% in Spain (American Action Forum, Cancer Care in the United States Is Unrivaled, April 2025). Cancer death rates have declined 33% since 1991 translating to approximately 3.5 million lives saved. US cancer mortality rates rank among the lowest of twelve comparable OECD countries.
Thirty-day mortality after heart attack, hemorrhagic stroke, and ischemic stroke is lower in the US than in many peer nations (Peterson-KFF Health System Tracker, October 2025). The FDA approved 50 novel drugs in 2024 alone.
Americans gain access to new therapies significantly faster than European and Canadian counterparts.
The US hosts a disproportionate share of global biomedical research, clinical trial infrastructure, and pharmaceutical innovation output (American Action Forum, April 2025; PMC10317843, 2023).
The Case for Saving Our System
The US market’s premium pricing, patent protection, and private sector R&D investment incentives produce approximately half of the world’s new drug approvals and host a disproportionate share of global biomedical research output. No peer system has demonstrated the capacity to generate comparable biomedical innovation at comparable scale.
This innovation engine is the one component of the US healthcare system the world cannot afford to lose.
How I Got Here
I opened this series unable to see a solution. The problems turned out to be more severe than I suspected, but also more precisely documented.
What changed was the framing. The failures are not random, they are identifiable points where financial conflict of interest drives decision-making processes. That specificity is what makes structural correction possible.
The proposals below are the product of this framework. I present them as coherent structural solutions, not as an ultimate ones.
If you enjoy evidence-based medical information, subscribe to receive these articles delivered to your mailbox every week.
The Reform Framework
Insurance Architecture
Creation of a new federal agency with a narrow mandate to establish uniform minimum coverage standards and standardized disclosure requirements nationally, enabling plan comparison at point of purchase. This will encourage increased insurance provider competition on all markets by removing state regulatory entry barriers in existence today.
Transition from direct to insurer government subsidies to a direct consumer one. Placing subsidy dollars on individual’s hands forces insurers to earn the customer with competitive offerings as precondition to accessing the subsidy.
When internal insurance appeal procedures are exhausted without resolution, the case proceeds to an independent review board composed exclusively of physicians with zero affiliation to the insurance industry. The board adjudicates on medical merit alone, decisions carry binding arbitration force.
The board’s aggregate reversal data feeds directly into the regulatory agency, where high reversal rates triggers company’s scrutiny of authorization practices. This becomes a new accountability process for repeat offenders.
Delivery Incentive Realignment
The AMA’s Relative Value Scale Update Committee is replaced by a fully independent government board with no institutional affiliations of any kind.
Primary care, preventive medicine, psychiatry, endocrinology receives reimbursement reflecting its actual clinical value and its demonstrated capacity to interrupt disease progression at lowest system cost.
A defined portion of existing Medicare Graduate Medical Education funding is reoriented toward primary care, preventive medicine, and psychiatry residency positions. GME reorientation and RVU re-weighting are explicitly linked interventions supporting the same goal.
Hospital Readmissions Reduction Program realignment applying a modest bonus for discharges within established length-of-stay parameters and more steep penalties for unjustified readmissions where the institution’s own discharge decision is the proximate cause.
Price Transparency With Enforcement
Mandatory publication of actual transaction prices for all elective and planned services, prescription drugs, and routine care, combined with financial penalties plus Medicare and Medicaid participation consequences for persistent non-compliance.
This will create the preconditions required for functional market competition in planned and elective care.
Pharmaceutical System Integrity
Upon FDA approval process request, the research budget transfers to an industry independent board which funds research development and completion by fully independent research teams. This applies across the entire drug lifecycle: pre-approval trials, post-market surveillance, and all required post-approval studies.
A foreign drug equivalent certification for identical products sold by the same manufacturer at lower prices in foreign markets, making them allowable for US insurance coverage.
Pharmacy Benefit Manager System
PBMs are compensated by transparent, per-transaction fees for clearly defined services eliminating the rebate system.
Only two members on a P&T committee are permitted to have any industry financial relationship. The rest are fully independent.
Mandatory PBM divestiture from any other healthcare related company that could create an operational conflict of interest.
Research Integrity and Clinical Standards
Medical society clinical practice guidelines derive validity from their adoption by CMS as the standard of care. As condition for adoption of new guidelines, CMS will require complete independence from any industry financial relationships from all clinical practice guidelines committee members.
CME Reform
CME accreditation requires that organizers and all presenters have no financial relationships with any healthcare industry entity. Unrestricted educational grants from industry to accredited CME organizations remain permissible.
Anti-Polypharmacy Initiative
A federally funded structured medication review program for Medicare beneficiaries delivers pharmacist-led, physician-supervised review with the explicit goal of identifying and safely reducing inappropriate polypharmacy burden.
Structured medication review reduces emergency department presentations by 27% (Christensen M et al., Cochrane Database of Systematic Reviews, 2016), is not associated with increased mortality in randomized trials and is associated with improved mental health and frailty outcomes (Page AT et al., British Journal of Clinical Pharmacology, 2016; PMC11182547, PLOS One, 2024).
Long-Term Care Infrastructure
A dedicated public long-term care benefit financed through defined payroll contribution during working years that activates on clinical need without the Medicaid spend-down requirement existing today.
Washington State’s WA Cares Fund represents the first domestic proof-of-concept for this model: implementation is ongoing, actuarial sustainability questions remain unresolved, and the experiment has not been in operation long enough to evaluate long-term outcomes (Washington State WA Cares Fund, official program documentation and actuarial analysis). The federal design should be informed by its results, not modeled on its current state.
The Food Environment
Metabolic disease dominates US healthcare expenditure. Its current trajectory will exhaust the healthcare budget if left unaddressed.
The FDA’s self-affirmation mechanism currently allows manufacturers to designate their own ingredients as generally recognized as safe (GRAS), a glaring conflict of interest. All GRAS designations will now require mandatory independent FDA review.
A defined portion of existing Farm Bill commodity subsidies can be reoriented toward whole food production from their current concentration in corn, soy, wheat, and sugar. This subsidy reorientation will contribute to lower whole food prices at the consumer level.
The Political Obstacle
Every proposal in this framework is legal, and feasible within existing governmental structures. All are achievable if the appropriate political will exists.
The political environment is not immovable. Whether it produces different political demands is outside any author’s control. What is within every reader’s control is whether or not they demand different behavior from the people who seek their vote.
Where This Ends
These proposals are not presented as the only possible answers. I do not hold them as correct answers in any final sense. They are meant to be the starting point for an open and constructive dialog.
I have now shared what forty years of observation and honest inquiry taught me.
Is the United State healthcare system worth saving? In my opinion… Yes! Provided changes addressing existing inadequacies are implemented.
The rest is up to you!
Found this article useful? Share your thoughts. Join the conversation below.
Educational content on The Metabolic Archives is free, because medical information should be accessible to everyone. If you find value and want to support the work, a paid subscription is available and genuinely appreciated. Visit the About Page for additional information.
The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.