
What’s Wrong with Medicine Today: My Perspective After Forty Years in the System
A Home Away from Home | Part Five

OPINION PIECE
When a hospital discharges a patient to a skilled nursing facility, most believe they are moving to the next stage of care. What they are actually entering is a separate industry, with its own financial architecture, staffing constraints, coverage rules, and incentive structure.

Menu of Post-Hospital Care Options
Skilled Nursing Facilities (SNFs) provide 24-hour nursing care, medication management, wound care, IV therapy, and short-term rehabilitation following hospitalization. They are the primary Medicare post-acute care setting.
Long-Term Care Facilities offer residential care for patients who cannot safely live independently due to chronic illness, cognitive impairment, or functional limitation. Medicaid is the primary payer for long-term residents. These facilities are frequently co-located with SNF units which creates confusion about the level of care on any given floor.
Inpatient Rehabilitation Facilities (IRFs) provide hospital-level rehabilitation for patients who can tolerate a minimum of three hours of active therapy per day. They are physician-directed, more heavily staffed than SNFs, and subject to stricter admission criteria.
Long-Term Acute Care Hospitals (LTACHs) serve patients requiring prolonged acute-level care — ventilator weaning, complex wound management, medically complex conditions — who no longer need the resources of an acute hospital but are not yet stable enough for SNF placement. They are the most clinically capable step-down setting and the least commonly available.
Home Health Services deliver skilled nursing and therapy in the patient’s home. They are designed for patients who are medically stable, functionally capable of managing basic needs with intermittent support, and living in an environment adequate to receive care.
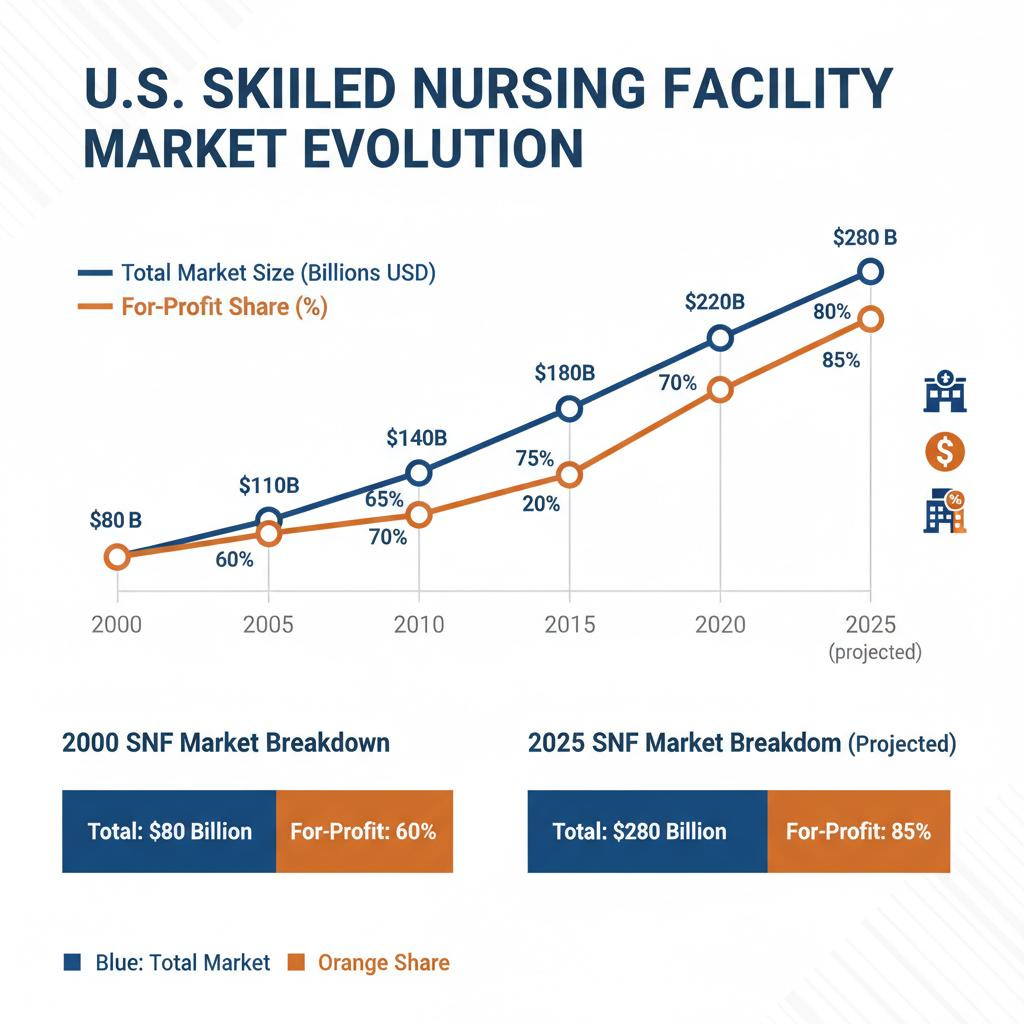
A $200 Billion Industry
The post-acute care market generated approximately $194 to $200 billion in revenue in 2024 and is projected to reach $290 billion by 2033 (Grand View Research, U.S. Skilled Nursing Facilities Market Industry Report, 2033; Future Market Insights, USA Skilled Nursing Facility Market 2025–2035). For-profit facilities now account for more than 70% of market share, driven by large corporate chains and private equity-backed operators.
What Private Equity Ownership Actually Produces
If you enjoy evidence-based medical information, subscribe to receive these articles delivered to your mailbox every week.
Following private equity acquisition of nursing home facilities, mortality during the facility stay and the subsequent 90 days increased 10% relative to non-private equity owned facilities, according to Gupta et al. (NBER Working Paper 28474, 2021), an analysis of Medicare data covering more than 7 million patients between 2000 and 2017.
Patients with cognitive problems in private equity-owned facilities were 50% more likely to be placed on antipsychotic medication. This lead to billing increases of 19% per stay driven by declines in staffing hours.
A 2025 analysis by AARP Florida examining 156 nursing home facilities following private equity acquisition found staffing declined 13%, facilities rated one star by CMS doubled from 10% to 21%, and five-star facilities dropped from 28% to 14% (AARP Florida, Change of Ownership and Quality in Florida Nursing Homes, 2025).
What These Facilities Are Actually Staffed to Deliver
Care is usually delivered by certified nursing assistants (CNAs), whose training is typically just weeks, under the supervision of licensed practical nurses (LPNs). Registered nurse (RN) oversight until recently was required only eight hours per day under federal standards (NursingHome411.org, citing CMS Final Rule on Minimum Staffing Standards for Long-Term Care Facilities, 2024). The remaining sixteen hours of the day, RN-level clinical assessment was not federally required to be present.
Higher RN staffing levels are associated with fewer pressure ulcers, lower restraint use, decreased infection rates, reduced inappropriate antipsychotic prescribing, lower mortality, and fewer emergency department visits and re-hospitalizations, findings consistent across multiple independent studies spanning decades (Harrington C, et al., Appropriate Nurse Staffing Levels for US Nursing Homes, Health Services Research, 2020, PMC7328494).
April 2024 CMS issued a rule that would have required 24-hour RN presence seven days per week, a change estimated to save 13,000 lives annually. The financial cost of providing 24-hour RN coverage was estimated at approximately $349 million annually across all facilities. The American Health Care Association and LeadingAge (the primary lobbying bodies for the nursing home industry) challenged the rule in federal court and in December 2025 CMS rescinded the requirement, reinstating the eight-hour standard.
The Service Gap
According to a federal analysis by the Assistant Secretary for Planning and Evaluation at HHS, if quality-optimizing staffing thresholds were implemented, 97% of all nursing home facilities would fail to meet one or more standards. A separate methodology in the same analysis estimated that 91% of nursing homes have nursing assistant staffing below minimal necessary care levels (ASPE HHS, State-Initiated Nursing Home Nurse Staffing Ratios: Annotated Review of the Literature).
In most SNFs, attending physician presence is limited to brief periodic visits, weekly or less frequent. Day-to-day clinical management falls to nursing staff, with physician availability by telephone. When a patient deteriorates acutely, the pathway to clinical intervention is considerably slower and less reliable than in an acute hospital.
The gap between what patients believe these facilities provide and what most of them are actually staffed to deliver is substantial. The clinical failures that follow are a predictable outcome.
Medicare Coverage and The Observation Status Trap
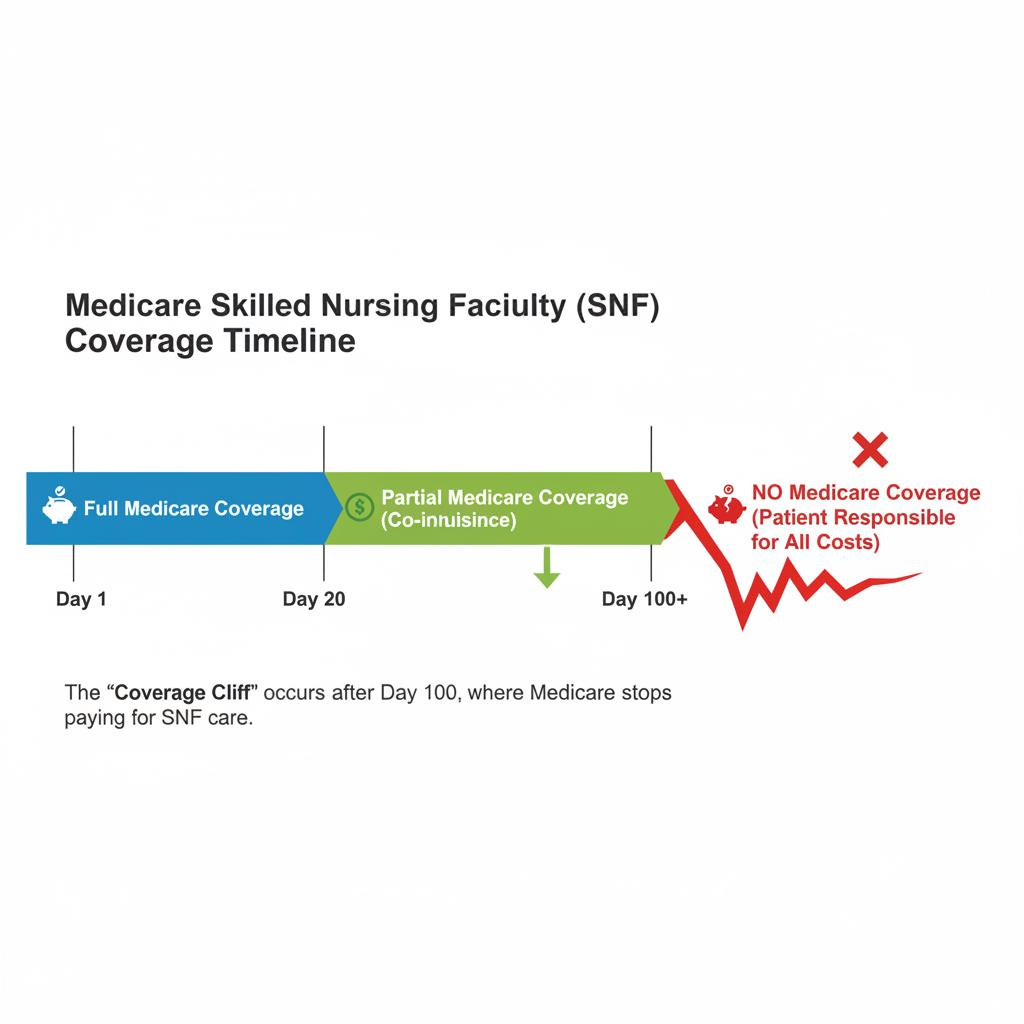
Medicare Part A covers SNF care at 100% for days 1 through 20 following a qualifying inpatient hospital stay of at least three consecutive days. Days 21 through 100 require a daily patient co-payment currently exceeding $200 per day, a cost most patients cannot sustain without supplemental insurance. After day 100, Medicare coverage ends entirely (Centers for Medicare and Medicaid Services, Skilled Nursing Facility Care Coverage, medicare.gov).
Medicare classifies observation status as outpatient care. Time spent under observation does not count toward the three-day inpatient requirement. A patient can spend four days in a hospital bed and have zero qualifying inpatient days if the hospital classified their stay as observation status (Center for Medicare Advocacy, Repeal the 3-Day Hospital Stay Requirement, September 2025; Society of Hospital Medicine, Observation Status: Current Issues).
The physician’s admission decision can be overruled retroactively by the hospital’s Utilization Review Committee, applying CMS criteria, frequently without physician input. The patient discovers the coverage consequence at discharge and the financial consequence can amount to thousands of dollars per day out of pocket.
Observation status carries a documented disparate impact on the poorest Medicare beneficiaries (Medicare Rights Center, Medicare Hospital Outpatient and Observation Status: The Three-Day Stay Problem, 2023). Neither the 2013 Two-Midnight Rule nor the 2015 NOTICE Act has resolved the problem. The decision that determines coverage is administrative.
SNF Coverage Window as a Billing Target
Within the covered period, the facility’s financial interest runs against early discharge. Every covered day generates revenue, discharging a patient before coverage ends foregoes that revenue. The patient who generated revenue on day 99 is a financial liability on day 101. The discharge that follows is calendar-determined. The question asked is not if the patient can safely transition home, is if coverage has ended.
Medicare patients discharged to SNFs face a 25% likelihood of readmission or death within 30 days. In a review of 200 SNF discharges, 67% of readmissions were rated as potentially preventable, with patients reporting that inadequate SNF treatment contributed to their returns (Mack D, et al., Implementation of a Skilled Nursing Facility Readmission Review Process, BMJ Quality and Safety, 2018, PMC6069909). The 25% readmission and mortality figure is consistent across multiple national analyses.
The Rehabilitation Therapy Billing Problem
SNF Medicare reimbursement was historically tied to the volume of rehabilitation therapy provided. This created a financial incentive to maximize therapy billing regardless of whether the patient was appropriate for or benefiting from it. Multiple large SNF chains faced federal fraud investigations and settlements related to therapy billing practices.
In 2019, CMS implemented the Patient Driven Payment Model (PDPM), replacing therapy-volume-based reimbursement with a model based on patient clinical characteristics (CMS, Patient Driven Payment Model, Implementation Documentation, 2019).
Choosing a Facility Under Pressure
The CMS Five-Star quality rating system exists and is publicly available. Staffing levels by shift are publicly reported but not easily accessible by a family at bedside. Private equity ownership is not disclosed in any standard admission document. The discharge planner’s recommended facilities may reflect network affiliation or bed availability rather than clinical fit.
A Word on Home Health
Home health is designed for patients who are medically stable, functionally capable of managing basic needs with intermittent support, and living in a home environment adequate to receive care. It is not continuous care and is not a substitute for the clinical monitoring of a facility setting.
The administrative discharge from a SNF to home health at coverage end, frequently places patients in a home health setting they may not be ready for yet. Home health’s own limitations mean the gap between what the patient needs and what home health can provide can be significant. The patient’s family then becomes the de facto care provider for most needs.
The System Is Working as Designed
The failures documented here are the predictable consequences of a system whose financial architecture has been allowed to operate with minimal accountability for clinical outcomes. A nearly $200 billion industry dominated by large corporate chains and private equity operators is a system that has been optimized for a purpose other than patient recovery.
Found this article useful? Share your thoughts. Join the conversation below.
Educational content on The Metabolic Archives is free, because medical information should be accessible to everyone. If you find value and want to support the work, a paid subscription is available and genuinely appreciated. Visit the About Page for additional information.
The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.
I'm finding that quality is no longer the norm in the medical field in general. It's all about getting paid. Great article though