
What’s Wrong with Medicine Today: My Perspective After Forty Years in the System
The Slow Death of the Independent Practitioner | Part Two

OPINION PIECE
An independent physician was a small business owner with one client: the patient. The physician’s income, and professional reputation depended entirely on the quality of care delivered to the person across the desk. The obligation ran directly from physician to patient, and nothing stood between them. The physician’s and the patient’s interest were aligned, this was the unspoken covenant at the center of the patient-doctor relationship.

The Arithmetic That Ended It
The financial equation of independent practice begin to fail as overhead grew faster than reimbursement, neither variable within the physician’s control.
Rising malpractice insurance, expanding administrative staff to manage billing complexity, the expanding coding infrastructure required by insurer and Medicare, electronic medical record systems mandated by federal law after 2009. These costs compounded over years while reimbursement rates from insurers and Medicare barely kept pace.
Medical practice is and shall always be a service business, anchored in the sacred relationship between doctors and patients. But when overhead outpaces revenue in any business, options are limited:
Increase prices — unfortunately the insurance pay model caps reimbursement with limited opportunity for price flexibility.
Add ancillary services — requires adequate staff capacity and access to capital for initial technology investment. Those costs plus your extra time investment need to be balanced against expected additional revenue produced, which is mostly determined by insurance reimbursement rates.
Reduce overhead — most of these are not entirely within the practice’s control.
Increase encounter volume — involves reducing time per patient visit, at the risk of trading quality for quantity.
Or, you can leave private practice entirely.
Around 1998 I transitioned to a hospital affiliated practice, in essence becoming a corporate employee. This practice allowed adequate time for meaningful patient encounters while the administrative burden of running a small business transferred to the institution. The trade seemed reasonable: give away some clinical autonomy in exchange for financial stability while upholding my personal patient care standards.
And for a while, it was.
If you enjoy evidence-based medical information, subscribe to receive these articles delivered to your mailbox every week.
What Health Coverage Actually Is
Health insurance is not insurance in the traditional sense. Traditional insurance covers low-probability, high-cost events: your house burning down, a car accident. The actuarial model works because most people never file a claim.
Health coverage is different. Every human being will consume healthcare, the only variables are timing and amount. This industry is basically a prepaid consumption mechanism operating inside an insurance’s legal structure.
When the Affordable Care Act eliminated several of the tools the industry had used to manage profitability under that structure — pre-existing condition exclusions, lifetime benefit caps, certain coverage exclusions — the industry rapidly adapted. Networks narrowed, deductibles rose, prior authorization expanded to areas not previously covered. Understanding this explains the experience patients have when dealing with a financial model trying to preserve its margin in a market where everyone eventually files a claim.
A National Wave
According to the Congressional Research Service, the portion of independent physicians fell from 57% in 2000 to 43% by 2009, with projections in 2012 already anticipating a further drop to 33% within a year (Congressional Research Service, Report R42880, 2013).
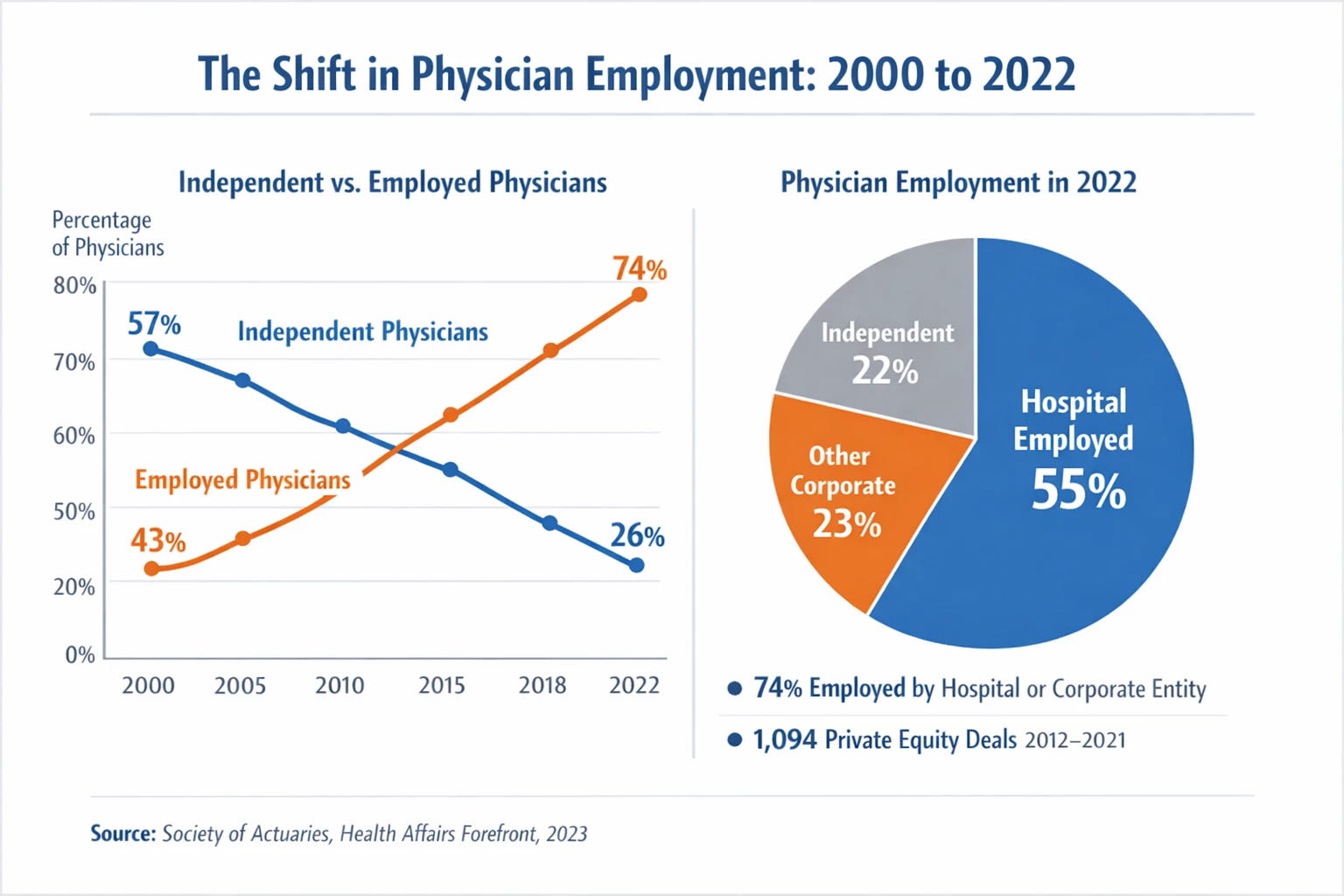
By 2022, 74% of all US physicians were employed by either a hospital system or another corporate entity. More than 55% are hospital-employed; another 23% work for other corporate owners, including private equity firms (Society of Actuaries, Health Care Provider Consolidation and Shortages, 2023; Health Affairs Forefront, 2023). Between 2012 and 2021, private equity firms completed 1,094 unique acquisition transactions involving US physician practices (Society of Actuaries, 2023).
The Same Pressures, New Instruments
The early years of hospital affiliated practice felt like a return to what medicine was supposed to be. The trade felt reasonable, but was not permanent.
As reimbursement constraints tightened against hospital overhead, the emphasis inside hospital systems shifted progressively from clinical outcomes to throughput. New targets appeared requiring increasing encounter numbers, intensified pressure to shorten hospital length-of-stay; the overall objective became discharging patients faster, freeing beds for the next paying clients. Discharge decisions gradually became logistical ones, driven mostly by the system’s needs.
Early throughput targets came with positive incentives: bonus compensation for meeting productivity benchmarks. What followed was financial penalties for failing to comply with the established targets. The moment the penalties materialized was the point the system crossed a line, a line my ethics and conscience could not cross.
My decision to retire was born out of that realization.
Who Bore the Cost
According to data presented at the American Heart Association’s 2025 scientific sessions, adjusted all-cause 30-day readmission rates increased for patients in the lowest and middle income quartiles between 2010 and 2019. During the same period, readmission rates decreased among patients in the highest income quartile (American Journal of Managed Care, November 2025). The federal Hospital Readmissions Reduction Program’s measured improvements in readmission rates were achieved disproportionately among wealthier patients.
Premature discharge hits those least equipped to self-manage between discharge and full recovery the hardest: those with limited financial resources, health literacy, support system at home, lacking the tools to navigate the complexities of our modern healthcare system.
While readmission data is observational, socioeconomic factors are themselves risk factors for readmission. The casual association between early discharge and increased readmission rates in this population, is both strong and consistent with my own anecdotal observations.
The Liability Trap
Prior authorization denials by insurance companies carry no formal malpractice exposure for the insurer. Discharge targets set by hospital administrators are not reviewed by medical boards. Corporate compensation structures that tie physician pay to bed turnover do not appear on the death certificate when a patient readmits and dies.
Full legal accountability still lands on the party whose clinical authority was systematically reduced. I want to be clear here: regardless of any pressure or constraints, physicians should be fully accountable for every clinical decision they make. However, when said decisions carry a threat of penalties from third parties with a financial interest in the results, it would be equitable to distribute the legal responsibility among all players involved.
Burnout Is Not a Wellness Problem
Depending on survey methodology and timing, between 48% and 58% of US physicians report burnout, significantly above the pre-pandemic baseline of approximately 40% in 2018 (AMA National Physician Burnout Survey, 2024; Physicians Foundation Survey, 2023; Stanford Medicine, April 2025). Among physicians still in training, the rate is 61%, and among medical students it is 71% (Physicians Foundation, 2023). In 2024 alone, 27% of medical groups reported a physician leaving or retiring early due to burnout (MGMA Stat Poll, September 2024).
A really somber statistic: more than half of US physicians know of a colleague who has considered, attempted, or died by suicide. One in five know of a colleague who has done so within the past twelve months (Physicians Foundation, 2023).
A Brief Acknowledgment
In 2020, physicians and nurses entered clinical environments they knew were dangerous, and did so knowing they lack adequate protective gear. They showed up because professional duty required it. Some of them never made it out; people I knew, friends, colleges.
What You Lost and May Not Been Able to Name
If you moved to an employed provider inside a health system in the past two decades, you probably experienced something different: shorter office visits, earlier hospital discharges, referral to institutional affiliated consultants and services.
What feels like a failure of the relationship between you and your doctor is a failure of the healthcare system. The physician is not withholding time and attention, is operating inside a system that has restructured both.
Found this article useful? Share your thoughts. Join the conversation below.
Educational content on The Metabolic Archives is free, because medical information should be accessible to everyone. If you find value and want to support the work, a paid subscription is available and genuinely appreciated. Visit the About Page for additional information.
The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.
Excellent summary! Such a complex mess. It should (and I believe could) be easier…
So sad about doctor's burnout and suicide! We need you!