
The Root System: A Complete Guide to Insulin Resistance
Part Three: The Body as a Network

This article and the next briefly explore some of the manifestations of metabolic syndrome, conditions we consider as individual but in reality are the result of a multi-systemic failure caused by underlying insulin resistance. In fact, a person afflicted by any of these conditions is likely to suffer from one or more conditions in this list. After all, they share a common pathological mechanism.
We will start with the quintessential metabolic condition: Type 2 Diabetes Mellitus.
Type 2 Diabetes Mellitus
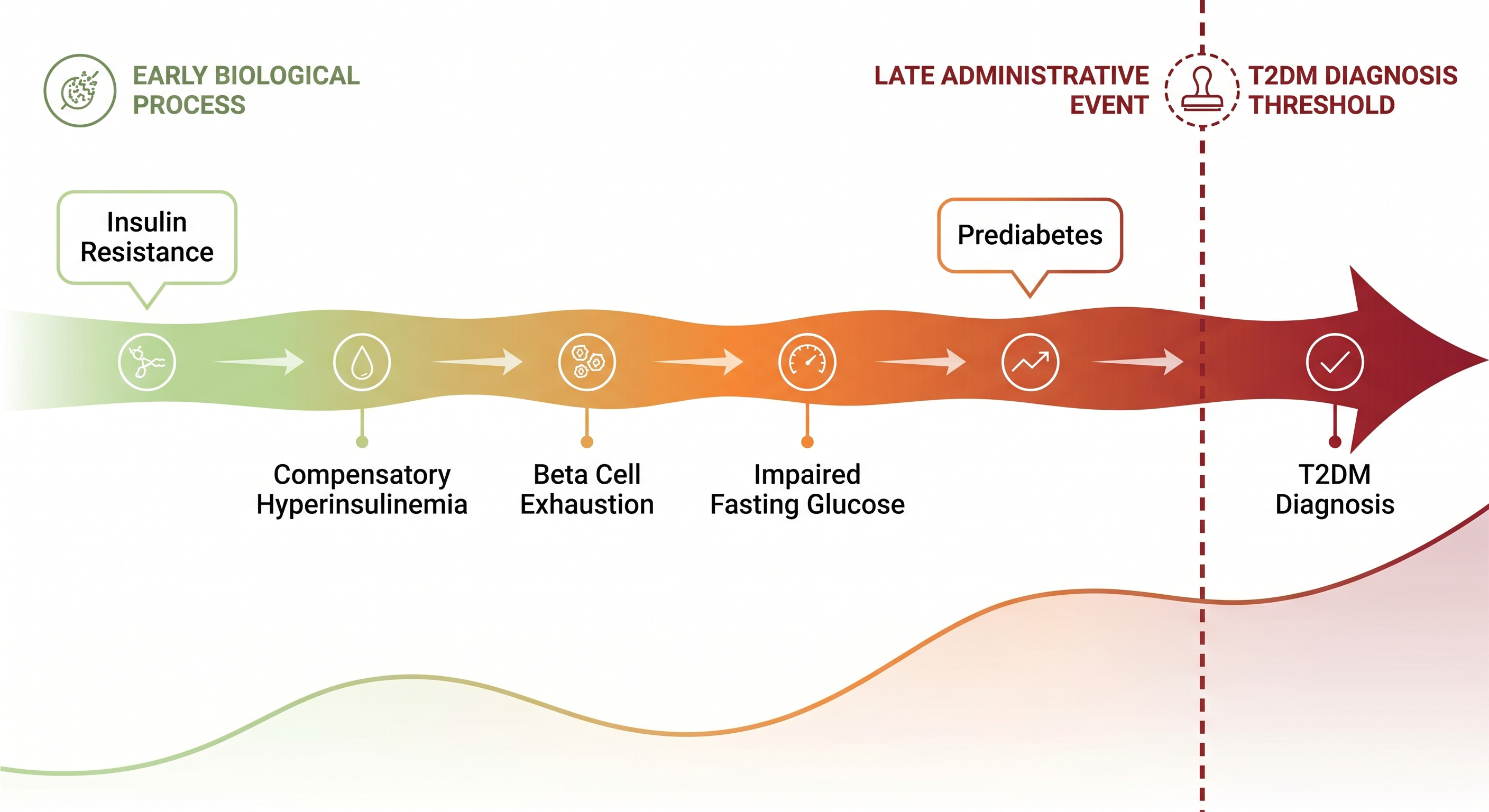
Diagnosis of Type 2 Diabetes Mellitus (T2DM) marks the moment when the body can no longer keep up with progressive insulin resistance. Glucose levels finally rise above normal. However, insulin resistance is an evolving process present but undetected for years, we call it pre-diabetes.
Accepted diagnostic criteria for diabetes as of the date of this article are:
Fasting Plasma Glucose (FPG) ≥126 mg/dL (7.0 mmol/L) after ≥8 hours of fasting
2-Hour Plasma Glucose (2hPG) during 75g OGTT ≥200 mg/dL (11.1 mmol/L)
HbA1c ≥6.5% (48 mmol/mol)
Random Plasma Glucose ≥200 mg/dL
The classic presenting symptoms include:
Polyuria — excessive urination
Polydipsia — excessive thirst
Polyphagia — excessive appetite
Unexplained weight loss
As of 2021, 537 million adults worldwide were living with diabetes, a figure projected to reach 783 million by 2045 (IDF Diabetes Atlas, 10th Edition, 2021). In the United States alone, approximately 96 million adults, about one in three, have pre-diabetes, and the majority are unaware of it (CDC National Diabetes Statistics Report, 2022).
Common complication of diabetes include: retinal damage leading to loss of vision, cardiovascular disease, stroke, erectile dysfunction, sensory and autonomic nerve damage, and several others. One complication deserving special attention: T2DM is the most common cause of non-traumatic lower extremity amputation in the USA.
Is important to realize that the inflammatory vascular damage responsible for most diabetic complications starts 5-10 years before a formal diagnosis, and progresses undetected during the pre-diabetic phase. Early diagnosis and aggressive lifestyle modification can stop and reverse disease progression.
Diabetes mellitus will be covered in detail on a separate series. The initial article is already published here.
Hyperlipidemia
When the liver becomes insulin resistant, it continues to overproduce very low-density lipoprotein (VLDL) particles while simultaneously impairing triglyceride clearance. Cholesteryl ester transfer protein activity depletes high-density lipoprotein (HDL) in exchange for triglycerides, and hepatic lipase remodels the remaining low-density lipoprotein (LDL) particles into the small, dense subtype that penetrates the arterial wall more readily and persists longer in circulation.
The result is the atherogenic dyslipidemic triad: elevated triglycerides, reduced HDL, and small dense LDL predominance, a pattern linked to hepatic insulin resistance and substantially more atherogenic than elevated LDL cholesterol alone (Taskinen and Borén, Atherosclerosis, 2015).
While standard lipid panels report total LDL cholesterol, they do not distinguish large buoyant LDL from small dense LDL. A patient with insulin resistance can return a total LDL within the normal range with a large portion of those being very dense LDL particles.
A future article will address the assessment and management of insulin resistance-driven dyslipidemia in full.
If you enjoy evidence-based medical information, subscribe to receive these articles delivered to your mailbox every week.
Obesity and Metabolic Syndrome
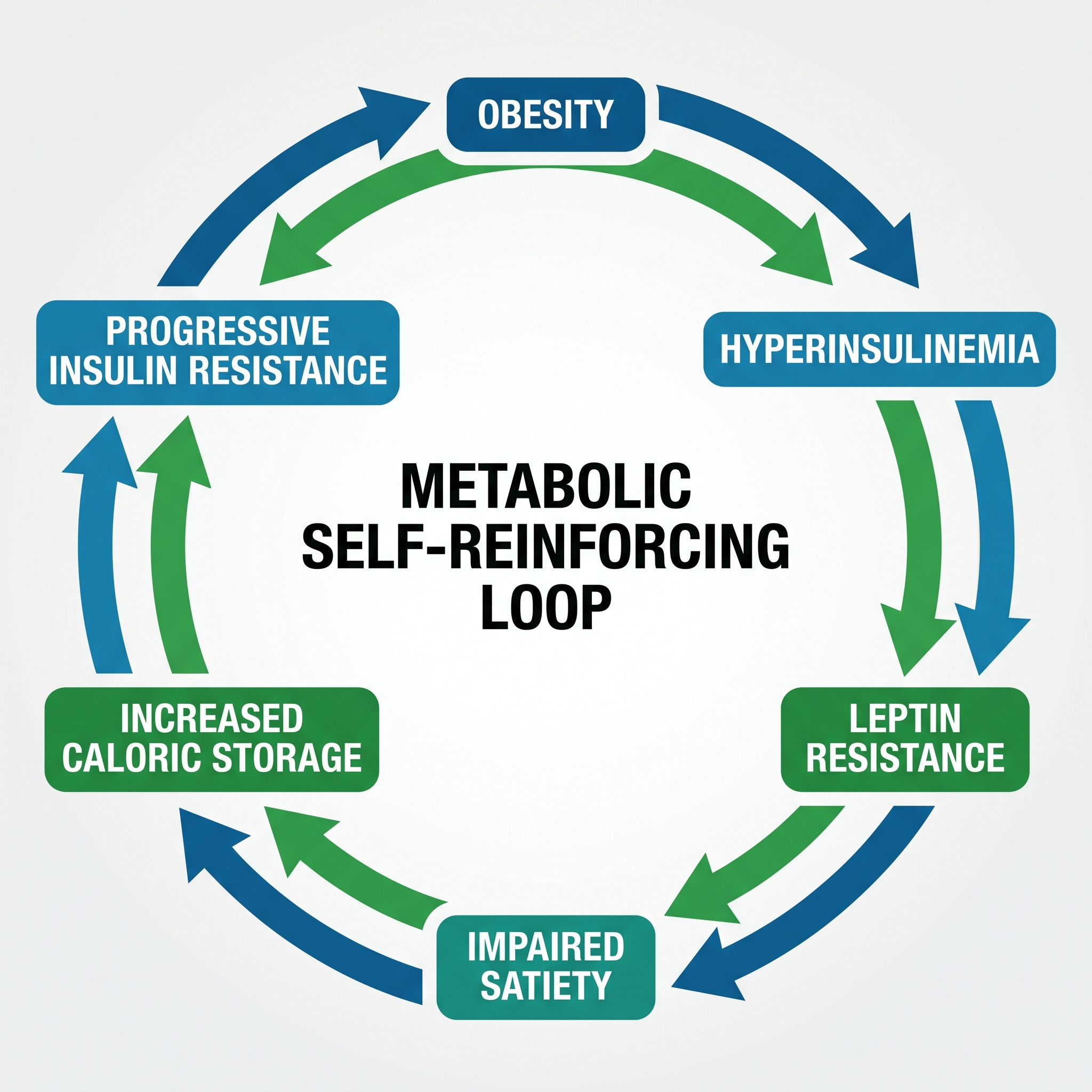
Excess adiposity, particularly visceral fat, releases free fatty acids and pro-inflammatory cytokines that directly impair insulin signaling at the receptor and post-receptor level. As insulin resistance deepens, compensatory hyperinsulinemia takes over and chronic hyperinsulinemia promotes fat synthesis and inhibits fat mobilization simultaneously.
Hyperinsulinemia also drives central leptin resistance, impairing the hypothalamic satiety signal that would otherwise prevent excess caloric intake. The result is a system that is simultaneously storing more fat, burning less of it, and receiving a progressively degraded satiety signal.
Metabolic syndrome is the clinical name for the point at which this process becomes visible, is defined by the presence of these five findings: abdominal obesity, elevated fasting triglycerides, reduced HDL cholesterol, elevated blood pressure, and impaired fasting glucose.
Obesity is more responsive to lifestyle modification at the early stages, when increasing subcutaneous fat is first detected. As abdominal (visceral) fat begins accumulating, the self sustaining mechanisms makes loosing weight more difficult the longer you wait to make changes.
Obesity is extensively discussed in two articles elsewhere on this site: Part One and Part Two.
Polycystic Ovary Syndrome
Insulin resistance is present in the majority of women with PCOS regardless of body weight (Teede et al., 2018). Lean women with PCOS carry the same underlying metabolic driver. The hyperinsulinemia-CYP17A1-ovarian androgen axis operates independently of obesity which is why the condition’s metabolic trajectory parallels insulin resistance severity.
Women with PCOS carry substantially elevated lifetime risk of type 2 diabetes, cardiovascular disease, and non-alcoholic fatty liver disease, because all of them share the same metabolic root. The main management for this condition is the diabetes drug metformin, it addresses some of the pathways leading to insulin resistance.
If you are pre-menopausal woman with abdominal fat accumulation you need to take this seriously. Start aggressive lifestyle modification and seek additional testing from your doctor: specifically sex hormone-binding globulin (SHBG) levels.
Hypertension
Arterial hypertension is usually not associated by most people as related to insulin resistance. While there are other causes of hypertension, if you have abdominal obesity, abnormal lipids and/or pre-diabetes, your hypertension is likely the result of underlying insulin resistance.
Different mechanisms lead to insulin resistance mediated arterial hypertension.
First, chronic hyperinsulinemia directly stimulates sympathetic nervous system outflow, raising heart rate and peripheral vascular resistance (Landsberg, Journal of Hypertension, 2001).
Second, insulin acts on the proximal renal tubule to enhance sodium-hydrogen exchanger activity, promoting sodium retention, volume expansion, and the pressure increase that follows (DeFronzo, Diabetologia, 1981).
Third, insulin resistance effects in the vascular endothelium is not uniform: the PI3K-eNOS-nitric oxide vasodilatory pathway is selectively impaired while the MAPK-endothelin-1 vasoconstrictive pathway is preserved. The net result is a shift in vascular tone toward vascular constriction (Muniyappa and Sowers, Reviews in Endocrine and Metabolic Disorders, 2013).
Fourth, visceral adipose tissue generates angiotensinogen locally, activating the renin-angiotensin-aldosterone system and adding a fourth independent pressure-elevating mechanism to the three already operating.
Conventional antihypertensive therapy mostly addresses the pressure reading. With the exception of ACEI/ARB class medications, most of these mechanisms are left unaddressed. If you have unexplained (often called essential) hypertension, ask your doctor for a lipid and pre-diabetes screening if you haven’t already. If visible obesity is already present despite normal laboratories, aggressive lifestyle modification needs to be an active part of your treatment.
An Unescapable Reality
The metabolic syndrome caused by a single underlying insult, insulin resistance, is one the most striking clinical manifestation illustrating the interconnected nature of the human body. We have come to think the human body as a collection of separate independent systems: nervous, cardiovascular, gastrointestinal, etc. We have treated diseases based on this foundation for years. The reality is that our body is a collection of tightly interconnected systems, a failure in one has measurable effects on every other.
Six organ systems remain: the heart, the kidneys, the liver, the airway during sleep, the brain, and the relationship between insulin resistance and malignant transformation.
Found this article useful? Share your thoughts. Join the conversation below.
Educational content on The Metabolic Archives is free, because medical information should be accessible to everyone. If you find value and want to support the work, a paid subscription is available and genuinely appreciated. Visit the About Page for additional information.
The Metabolic Archives is for educational and informational purposes only, and is not intended as medical advice, diagnosis, or treatment, and does not constitute a doctor-patient relationship. Do not adopt any recommendation discussed in any article or guides published here, make changes or abandon any prescribed medical treatment without prior consultation with your physician. Always seek the advice of your physician or other qualified health provider for any questions regarding your medical condition and recommended treatment options.
By reading this post, you acknowledge that you have read and agree to the Terms of Service of The Metabolic Archives, which govern all use of this content including restrictions on reproduction.
© 2026 The Metabolic Archives. All rights reserved.
Tags: insulin resistance, metabolic syndrome, type 2 diabetes, PCOS, hypertension, dyslipidemia, obesity, patient education